Insidious Onset of Localised Small Intestinal Perforation by Ingested Plastic Fork
By Serhan Yilmaz1, Husnu Aydin2, Hakan Bolukbasi1Affiliations
doi: 10.29271/jcpsp.2022.08.1070ABSTRACT
Ingestion of a foreign body is generally observed in the psychiatric patients and children. Healthy adult individuals may also swallow a foreign body unintentionally. Here, we report a case of a patient who swallowed a plastic fork and treated with laparoscopic repair. A 46-year man was admitted to the emergency room with the abdominal pain. His physical evaluation and diagnostic imaging revealed free air in the abdomen. Further imaging with CT scan showed a foreign body in the proximal ileum. On taking details of his swallowing history, he remembered swallowing a broken part of a plastic fork unwittingly during dinner. Following the removal of the foreign body, the perforation area was primarily repaired in double layers. The postoperative course was uneventful. An accurate diagnosis of the small intestinal perforation caused by the ingested foreign bodies, particularly in cases where the patient is unaware of the ingestion, can be difficult. CT scan is a useful tool when available to establish the diagnosis before the surgical intervention.
Key Words: Small intestine, Perforation, Foreign body, Laparoscopic surgery.
INTRODUCTION
Plastic utensils, the use of which has been increasing in industrial societies can lead to the unexpected complications if not used carefully. Although accidental ingestion of the foreign bodies is generally seen in the psychiatric patients and children, healthy adult individuals may also swallow a foreign body unintentionally.
The foreign bodies are excreted through the stool by passing through the gastrointestinal system (GIS) within a week without causing any complications. However, rare major complications such as obstruction, hemorrhage, or perforation may occur depending on the nature, size, and shape of the foreign body.1 Perforation due to the foreign body ingestion occurs in less than 1% of all the patients and the most common site has been reported to be terminal ileum in 38.6%.1 Delay in the diagnosis may occur depending on the non-specific clinical findings and the latent period till the formation of perforation.2
Here, we present a case of an adult male with ileal perforation due to the foreign body ingestion who was treated through laparoscopic surgery.
CASE REPORT
A 46-year male patient was admitted to the emergency department with abdominal pain that had been ongoing for two days. On examination, the patient was orientated, cooperative, and conscious. Arterial blood pressure was 120/80 mmHg and pulse was 70 beats/minute. During the physical examination, tenderness and voluntary contraction were noted in the left lower quadrant. White blood cell (WBC) count was 20,092/mm3 and C-reactive protein (CRP) was 8.58 mg/L. No abnormal findings were observed in plain abdominal radiographs.
Computed tomography (CT) was performed upon the identification of edema in the descending colon wall and haustral thickening in abdominal ultrasonography (USG) and the continuation of the patient's abdominal examination findings. The CT revealed a foreign body in the lumen perforating the intestinal wall to the level of the small intestine and there was a small amount of free air around the intestine (Figure 1).
In the laparoscopic exploration performed under emergency conditions, the mesenteric side of the small bowel loop located 180 cm distal to the ligament of Treitz and omentum was seen to contain the perforation area. There was no intra-abdominal free intestinal or bile fluid. The foreign body causing perforation was a pointed plastic piece with a length of about 3-4 cm. Following the removal of the foreign body, the perforation area was primarily repaired in the two double layers. It emerged from the history that the patient had eaten food with a plastic fork two nights ago and unwittingly swallowed the broken part of it.
A relatively early diagnosis was made for the patient, who had no clinical signs of acute abdomen, by using imaging methods and the operation was completed laparoscopically (Figure 2). On the third day after the operation, the patient was discharged without any complications.
 Figure 1: Axial computerised tomography scan showing the foreign body and appearance of free air in the abdominal cavity.
Figure 1: Axial computerised tomography scan showing the foreign body and appearance of free air in the abdominal cavity.
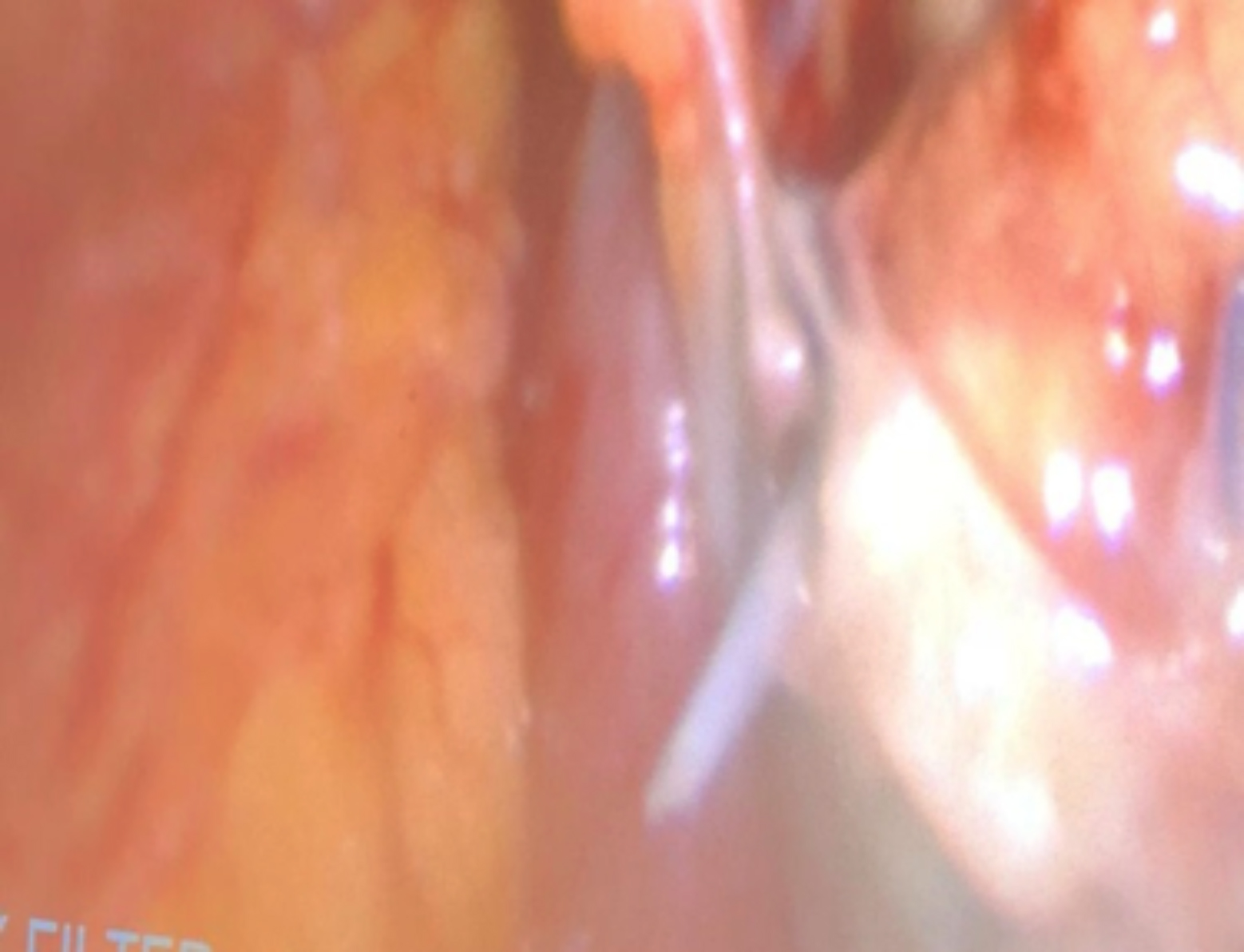 Figure 2: Laparoscopic intraoperative image of the plastic fork where it perforated the intestine.
Figure 2: Laparoscopic intraoperative image of the plastic fork where it perforated the intestine.
DISCUSSION
Foreign body ingestions can rarely cause complications such as perforation, obstruction, and hemorrhage.2 It may be more difficult to detect complications and to make a correct diagnosis, particularly in cases where the foreign body is swallowed unintentionally.
Although it is more common in paediatric, geriatric, and psychiatric patients, cases of accidental foreign body ingestion can be observed in the healthy adult population as in the present case.3
Chicken bones, fish bones, and toothpicks are the most common foreign bodies that cause perforation.4 Plastic forks, the use of which has been increasing in our daily lives, may also break and be accidentally ingested by the individual causing perforation in the gastrointestinal tract as in the present case.
In general, foreign bodies with a length of <6 cm and a width of <2 cm are excreted through faeces without causing any complications.5 The incidence of perforation caused by the ingested foreign body has been reported to be 1%. Due to the anatomical reasons, perforation occurs most frequently in the esophagus, ligament of Treitz, terminal ileum, ileocecal valve, and rectosigmoid junction.1,2 Perforation was at the proximal ileum level in the present case.
The sharp-edged foreign bodies may be impacted following the intestinal mucosal erosion or many penetrate into the peritoneal cavity by piercing the intestinal wall. Intra-abdominal free air or fluid may not be seen since the foreign body progressively produces erosion after being impacted into the intestinal wall and the perforation site is covered by the fibrin, omentum, and adjacent loops of the bowel.6 In this case, patients may present with an acute abdominal pain however, different complications such as localised or generalised abscesses, fistula formations, proctitis, omentitis, acute intestinal obstruction, and bleeding can also be seen.2
Various imaging techniques can be used for the early and accurate diagnosis. Factors such as intestinal leakage, low amount of free air, spontaneous closure, and absorption of free air reduce the appearance of free air below 50% in direct radiographs.2 Metallic foreign bodies can be seen on direct radiographs, but foreign bodies that are not radio-opaque may not be visible on direct radiographs. The obstruction-related findings can be observed in direct radiographs. The USG technique can be useful in detecting intra-abdominal fluid and in eliminating other diagnoses. For foreign bodies that are not radio-opaque, changes in tissues surrounding perforation area and luminal contents of superficial intestinal loops can be demonstrated via USG.7 The whole gastrointestinal system (GIS) can be evaluated via CT in detail. Thus, it can be used to detect the foreign body, the state of the perforation area, and the surrounding tissues.2 As in the present case, it can detect small amounts of free air outside the lumen.
Endoscopy can be used to remove and treat foreign bodies in the esophagus, stomach or large intestine.8 Observation, medical treatment, and radiological interventions can be tried in the presence of foreign bodies-related complications such as abscess, fistula, or ileus. Surgery is the gold standard treatment for foreign body-related perforations.9 In the present case, laparoscopic debridement and primary repair were performed for the perforated area since there was no peritoneal contamination and the patient's hemodynamical status was stable.
The mortality and morbidity rates have been reported to be 6.1–6.5% and 24–57% in foreign body-related small intestinal perforations, respectively.1-4 In these cases, the laparoscopic approach is a safe and effective method if performed by the experienced hands.10 The operation of our patient was completed laparoscopically and he was discharged without any complications on the third day following the operation.
In conclusion, small intestinal perforation caused by the ingested foreign bodies may lead to the high morbidity and mortality, particularly in cases where the patient is unaware of the ingestion. It is difficult to diagnose due to its slow and insidious course and highly variable symptoms. Diagnostic modalities, like CT, help in the early diagnosis and decision-making to prevent a poor outcome.
PATIENT'S CONSENT:
Written informed consent was obtained from the patient and the family to report this case study.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS' CONTRIBUTION:
SY, HA, HB: Involved in the conception, design and interpretation, wrote the manuscript, collected data, reviewed relevant published reports, and provided the images. Read and approved the final manuscript.
REFERENCES
- Goh BK, Chow PK, Quah HM, Ong HS, Eu KW, Ooi LL. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg 2006; 30(3): 372-7. doi: 10.1007/s00268-005-0490-2.
- Coulier B, Tancredi MH, Ramboux A. Spiral CT and multidetector-row CT diagnosis of perforation of the small intestine caused by ingested foreign bodies. Eur Radiol 2004; 14(10):1918-25. doi: 10.1007/s00330-004-2430-1.
- Velitchkov NG, Grigorov GI, Losanoff JE, Kjossev KT. Ingested foreign bodies of the gastrointestinal tract: Retrospective analysis of 542 cases. World J Surg 1996; 20(8):1001-5. doi: 10.1007/s002689900152.
- Rodriguez-Hermosa JI, Canete N, Artigau E, Girones J, Planellas P, Codina-Cazador A. Small bowel perforation by an unusual foreign body. Rev Esp Enferm Dig 2009; 101(9):639e641. doi: 10.4321/s1130-0108200900090 0007.
- Byrne WJ. Foreign bodies, bezoars, and caustic ingestion. Gastrointest Endosc Clin N Am 1994; 4(1):99-119. PMID: 8137021.
- Madrona AP, Fernandez-Hernandez JA, Carasco M, Carasco Pratas M, Riquelme J, Paritta Paricio P. Intestinal perforation by foreign bodies. Eur J Surg 2000; 166(4):307-9. doi: 10.1080/110241500750009140.
- Coulier B. Diagnostic ultrasonography of perforating foreign bodies of the digestive tract. J Belge Radiol 1997; 80(1):15. doi: 10.1080/110241500750009140.
- Hu J, Sun S. Endoscopic ultrasound-guided retrieval of a toothpick embedded in the stomach wall. J Clin Ultrasound 2017; 45(9):603-4. doi: 10.1002/jcu.22466.
- Brian KP, Goh BK, Chow PKH, Quah HM, Ong HS, Eu KW, et al. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg 2006; 30(3): 372-7. doi: 10.1007/s00268-005-0490-2.
- Govind G, Siriwardana HPP, Sdralis E, Ram M, Lee P, Charalabopoulos A. Chronic ileitis with transmural migration of ingested foreign body treated by laparoscopy. Acta Chir Belg 2018; 118(5):1-5. doi: 10.1080/00015458. 2017.1376432.