Serum Protein Electrophoresis and Immunofixation Electrophoresis Detection in Multiple Myeloma
By Shanshan Zhu, Wei Li, Meilin Lin, Tiemin LiAffiliations
doi: 10.29271/jcpsp.2021.07.864ABSTRACT
The objective of this study was to investigate the diagnostic significance of serum protein electrophoresis and immunofixation electrophoresis detection in diagnosis of multiple myeloma (MM). One hundred and five patients were investigated. The detection rate of M protein by immunofixation electrophoresis detection was better (105 cases, 100%) than that of serum protein electrophoresis (101 cases, 96.19%, p<0.001). The M band was not detected by serum protein electrophoresis in four cases (3.81%), among which one case (0.95%) was identified as IgA type and 3 cases (2.86%) as light chain type after immunoglobulin analysis. Immunofixation electrophoresis detection technique can be used for screening M protein in patients with atypical MM; and immunofixation electrophoresis detection technique can increase the diagnosis accuracy in patients with atypical MM.
Key Words: Multiple myeloma (MM), Serum protein electrophoresis, Immunofixation electrophoresis, Monoclonal immunoglobulin.
Multiple myeloma (MM) is a malignant clonal proliferating disease of plasma cells.1 The onset of MM is slow, and the common clinical symptoms include multiple osteolytic damage, anemia, infection and renal function damage. Clinical manifestations are diverse, but lack the specificity. The monoclonal proliferation of malignant plasma cells can produce a large number of monoclonal immunoglobulin (M protein).2 M protein is characteristic in patients with MM.
However, M protein is not produced in all MM. MM not producing M protein is called nonsecretory MM, which is rare and the prevalence rate is low. MM secreting M protein can be divided into IgA, IgG, IgM, IgD or IgE, according to the type of monoclonal immunoglobulin as well as light chain type dominated by free monoclonal light chain (k or λ) dysplasia.
MM is easily missed or misdiagnosed. There are many methods for clinical diagnosis of MM, such as X-ray examination, bone marrow cytology examination, urine Bence-Jone protein, and erythrocyte sedimentation rate. As the changes of bone marrow and bone in patients with early MM are not obvious, the positive rate of X-ray in the diagnosis of MM is high.3 Bone marrow cytology examination requires multiple punctures, which makes patients suffer and lead to limited application.
The positive rate of urine Bence-Jone protein in the diagnosis of MM is low. Although the positive rate of erythrocyte sedimentation rate in the diagnosis of MM is high, the specificity is low. Therefore, it is necessary to actively find a more accurate and painless diagnostic method.
Serum protein electrophoresis refers to the separation of different types of proteins, according to the differences in the surface charge of serum proteins, and the analysis of the changes in protein levels. Thus, judging the condition of patients' body. The full view of plasma protein can be obtained by serum protein electrophoresis. Studies have shown that serum protein electrophoresis can be as one of the diagnostic tools of MM.4 Immunoglobulin (Ig) is a class of immunoreactive molecules with tetrapeptide chain structure, which can be divided into five categories: IgA, IgM, IgD, IgE, or IgG. The level of serum Ig will change in MM patients, which can be used in diagnosis of MM. Therefore, the application of serum immunofixation electrophoresis detection technology in the diagnosis of MM has also attracted attention. The principle of immunofixation electrophoresis is the combination of the dissociation of electrophoresis and the high specificity (antigen-antibody reaction) and high sensitivity of monoclonal immunoglobulin to detect monoclonal components in serum.
The purpose of this study was to investigate the diagnostic significance of serum protein electrophoresis and immunofixation electrophoresis detection in the diagnosis of MM.
This descriptive study was approved by the Ethics Committee of Affiliated Hospital of Hebei University, China. A total of 105 patients with MM diagnosed from March 2019 to May 2020 were included. A total of 105 patients with MM were included. The diagnostic criteria of MM were that bone marrow detection showed that plasma cells were above 15%, abnormal plasma cells were found, and plasma cell tumors were diagnosed by tissue biopsy; serum detection showed that there was monoclonal Ig (M protein), and IgG index was above 35g/L, IgA index above 20g/L and IgM index above 15g/L; and there were osteolytic lesions or extensive osteoporosis symptoms. All the cases met the diagnostic criteria of MM. The inclusion criteria were diagnosed MM patients with informed consent. The exclusion criteria were pregnant women, patients complicated with liver disease, hematopathy, nephropathy, malignant tumor, rheumatism or other diseases influencing immunofixation electrophoresis detection, and patients with mental illness.
Three mL venous blood was collected on fasting and then separated within two hours to avoid hemolysis and lipid blood. The M protein bands in the serum were detected by agarose gel electrophoresis.
The method of serum immunofixation electrophoresis was that patients’ serum and 0.9% sodium chloride solution were mixed and diluted according to the proportion of 1:5; and 17 µL were taken from each sample to perform sampling point at five five different positions on AGAR plate. Serum proteins were separated by electrophoresis, according to their difference in electric charge. IgA, IgM, IgG, λand k antiserums were respectively added into the five electrophoresis zones in proper order. They were incubated on AGAR plate for 10 mins to remove excess antiserums, and then dried. After protein fixation, running gel was rinsed in eluant to eliminate unbinding proteins and make antigen-antibody complex remain on AGAR plate.
Then, it was dyed, discolored and dried. Finally, it was scanned, and the results were observed and recorded.5
SPSS version 25 was used for data analysis. The categorical data were expressed by n (%). Kolmogorov-Smirnov test was used to test the normality of data. Normally distributed data was represented as mean ± S.D. Categorical data for detection rate of M protein by immunofixation electrophoresis detection and serum protein electrophoresis were compared by the McNemar’s test. A p-value less than 0.05 was regarded as statistically significant.
Among the 105 patients, there were 62 males (59.05%) and 43 females (40.95%); with an average of 61.77 ± 10.83 years; and the disease duration with an average of 6.73 ± 1.01 months.
The results of serum protein electrophoresis showed that among the 105 MM patients, 101 cases (96.19%) were positive for M band and 4 cases (3.81%) were not detected. Among the 101 cases with positive M-band, 93 cases were located in the γ region, two cases in the β region, and six cases between the β and γ region. The positive M-band and the location were shown in Figure 1a and 1b.
The positive rate of M protein was 100% in the 105 patients with MM diagnosed. The detection rate of M protein by immunofixation electrophoresis detection was 105 cases (100%), which was higher than that of serum protein electrophoresis 101 cases (96.19%, p<0.001). The M band was not detected by serum protein electrophoresis in four cases (3.81%), among which one case (0.95%) was identified as IgA type and three cases (2.86%) as light chain type after immunoglobulin analysis.
The results of immunofixation electrophoresis detection showed that the monoclonal band (M band) was a narrow, dense, concentrated and clearly bounded precipitation band, which was in the same horizontal position as the M band on the reference lane (ELP). Figure 1c and 1d show a common type of electrophoresis map.
According to the results of immunofixation electrophoresis detection, among the 105 patients, type IgG was the most (60 cases, 57.14%), of which 31.43% was type κ and 25.71% was type λ; and type IgA took the second place (27 cases, 25.71%), of which 13.33% was type κ and 12.38% was type λ, as shown in Table I.
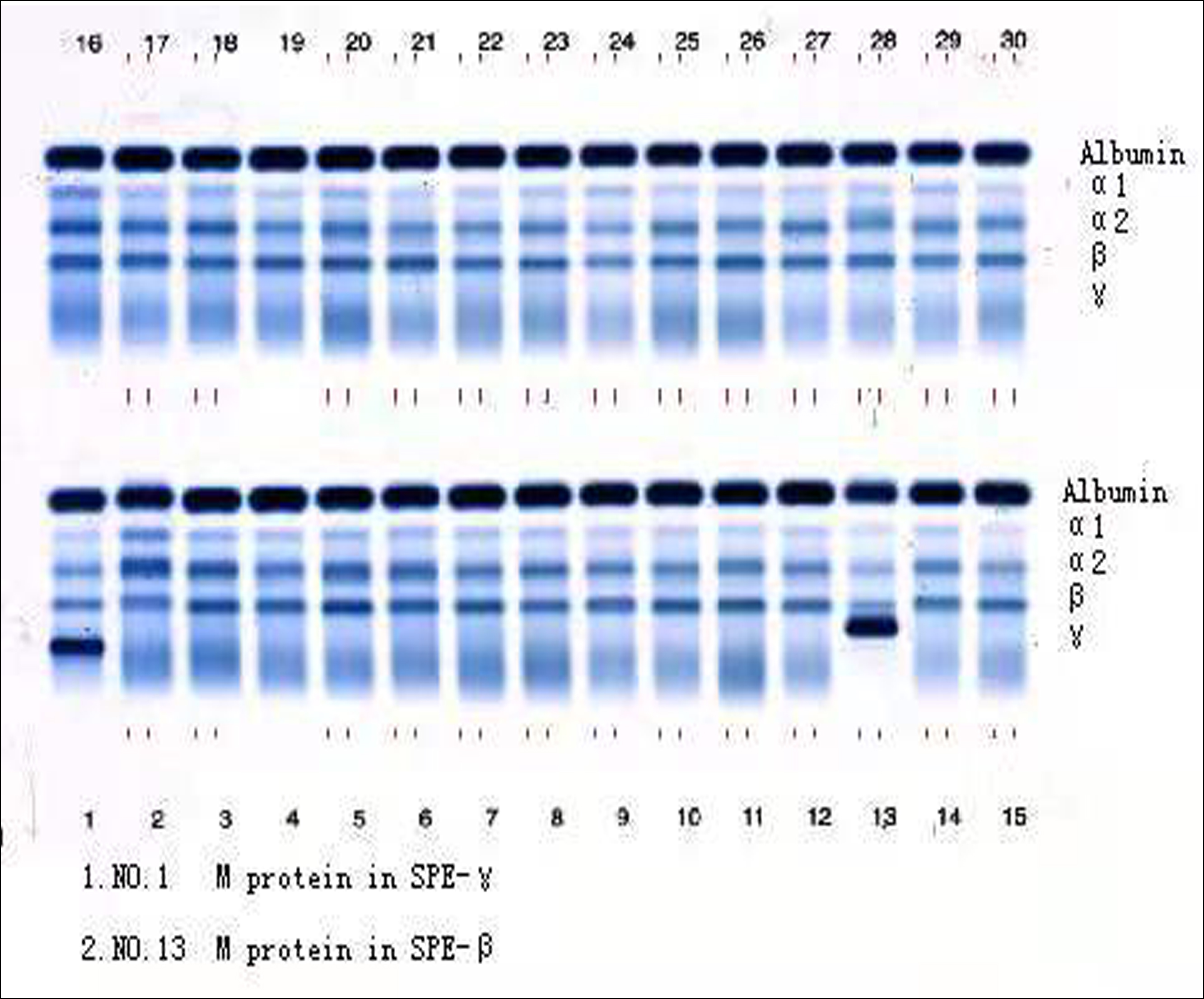 Figure 1a: M protein in SPE-γ and β.
Figure 1a: M protein in SPE-γ and β.
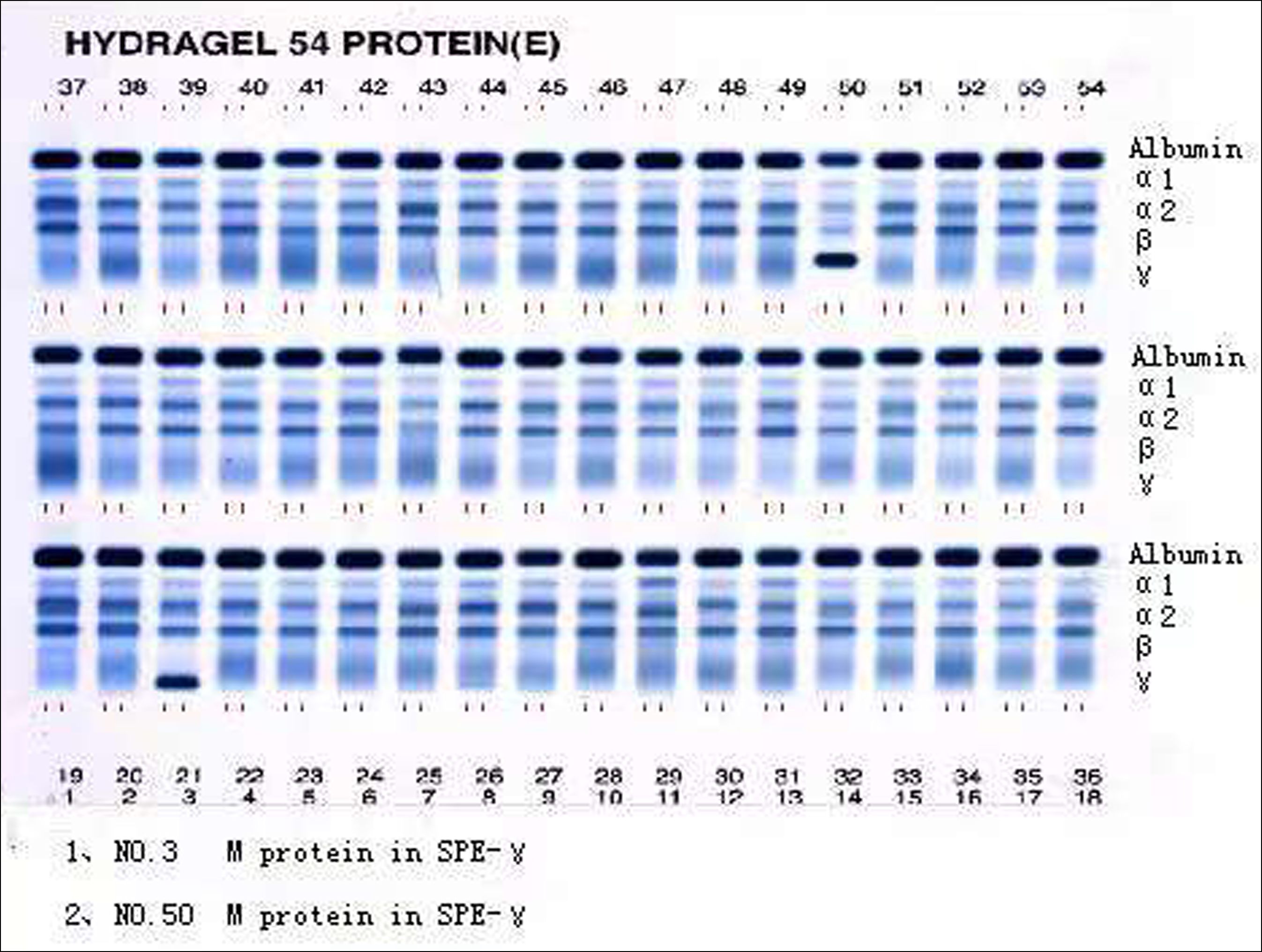 Figure 1b: M protein in SPE-γ.
Figure 1b: M protein in SPE-γ.
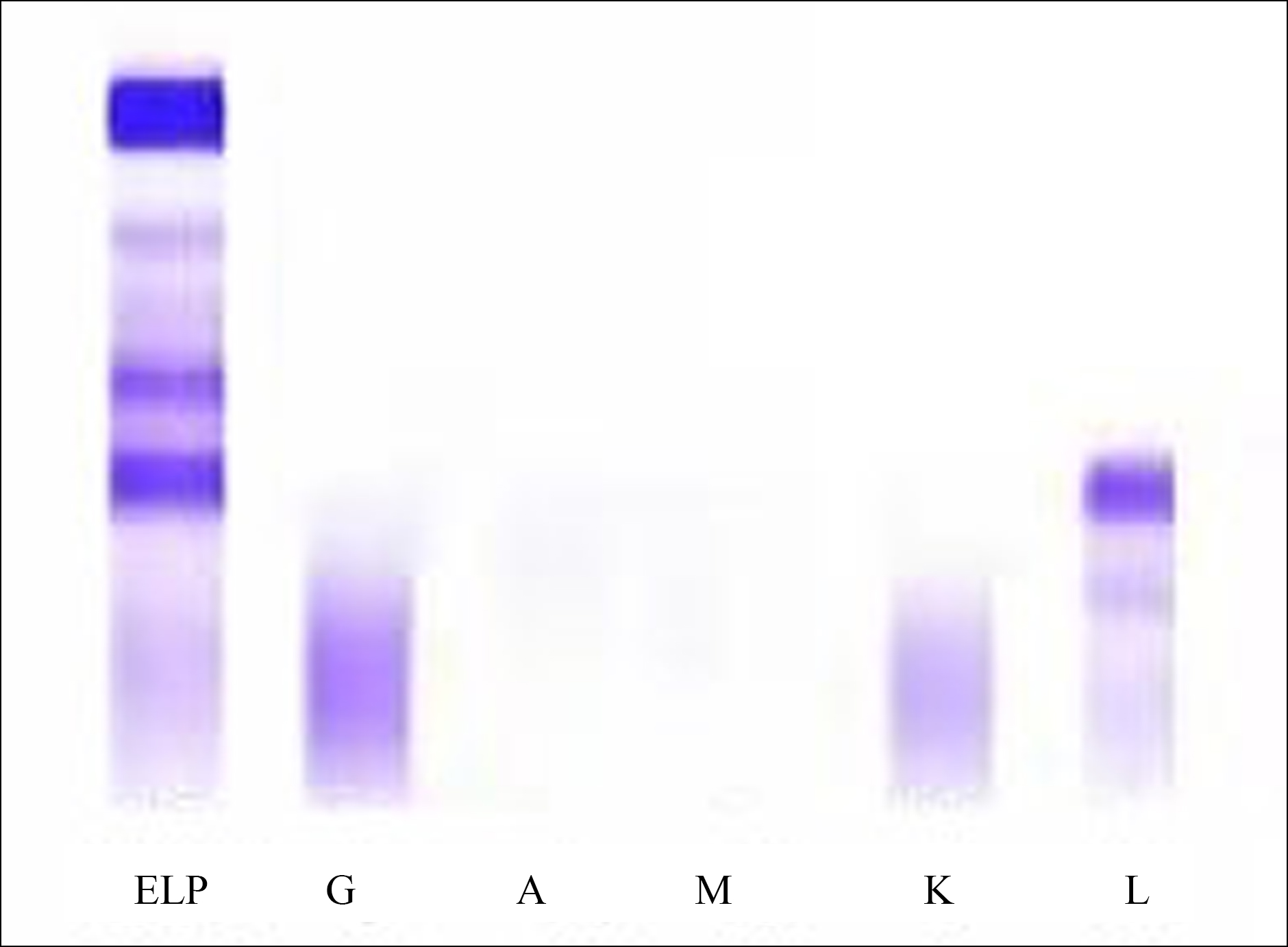 Figure 1c : Positive serum light chain Lambda.
Figure 1c : Positive serum light chain Lambda.
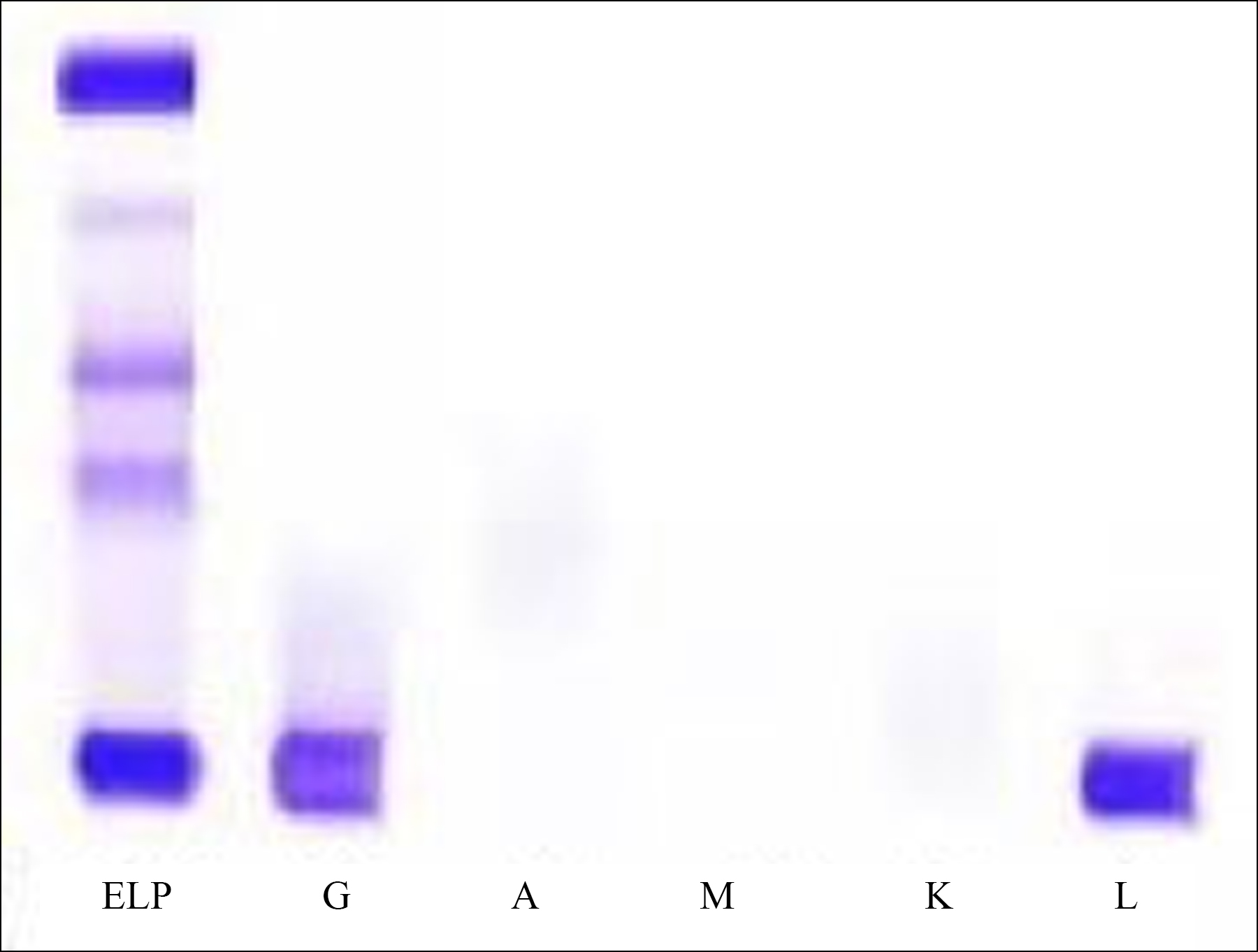 Figure 1d: Positive serum IgG-Lambda.
Figure 1d: Positive serum IgG-Lambda.
Table I: Types of serum immunofixation electrophoresis detection in the 105 patients.
|
Immunophenotyping |
Type k [ (n(%) ] |
Type λ [ (n(%) ] |
Total [ (n(%) ] |
|
Type IgG |
33 (31.43) |
27 (25.71) |
60 (57.14) |
|
Type IgA |
14 (13.33) |
13 (12.38) |
27 (25.71) |
|
Type IgM |
9 (8.57) |
6 (5.71) |
15 (14.29) |
|
Light chain type |
1 (0.95) |
2 (1.90) |
3 (2.86) |
|
Total [ (n(%) ] |
57 (54.29) |
48 (45.71) |
105 (100.0) |
This study showed that the positive rate of M protein was 100% in the 105 MM patients. It is suggested that all the subjects in this study produce M protein, and no nonsecretory MM is found. The detection rate of M protein by immunofixation electrophoresis detection was 105 cases (100%), which was higher than that of serum protein electrophoresis 101 cases (96.19%). The McNemar’s test result showed that the difference between the two groups was statistically significant. This study collected the cases with confirmed MM, using the method of retrospective case data analysis, and the sample size was small, so the conclusion of this study needs to be further verified by a large sample population. It should be noted that serum protein electrophoresis has limitations in the diagnosis of secretory light chain MM. The operation of immunofixation electrophoresis and the judgment of results need experienced professionals.
In addition, immunofixation electrophoresis detection was used to identify serum M protein in the 105 patients with MM. The results showed that IgG type (60 cases, 57.14%) was the most, including 31.43% type κ and 25.71% type λ, and type IgA (27 cases, 25.71%) took the second place, including 13.33% type κ and 12.38% type λ. It is suggested that immunofixation electrophoresis detection technique can directly identify the type of M protein with high sensitivity and specificity, which can be used as a routine detection method for MM. The conclusion of this study is consistent with the report of Yan.6
In conclusion, it is said that serum protein electrophoresis and immunofixation electrophoresis detection can be used in the diagnosis of MM, and both have their own advantages.
ETHICAL APPROVAL:
This study was conducted with the approval from the Ethics Committee of Affiliated Hospital of Hebei University, China.
PATIENTS’ CONSENT:
All patients signed a document of informed consent.
CONFLICT OF INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
SZ: Interpretation of data for the work, writing, and revising the work.
WL: Data collection, statistics and discussion.
ML: Helped perform the analyses with constructive discussions.
TL: Led and conceived the project, and final approval of the version to be published.
REFERENCES
- Fatima S, Ijaz A, Khan DA, Fatima F, Asif N, Hafeez A, et al. Cost-effectiveness of screening and confirmatory tests for multiple myeloma in Pakistani population: An audit report. J Coll Phys Surg Pak 2018; 28(7):560-3. doi: 10.29271/ jcpsp.2018. 07.560.
- Sidiqi MH, Aljama M, Kumar SK, Jevremovic D, Buadi FK, Warsame R, et al. The role of bone marrow biopsy in patients with plasma cell disorders: Should all patients with a monoclonal protein be biopsied? Blood Cancer J 2020; 10: e333. doi.org/10.1038/s41408-020-0319-0.
- Hinge M, Andersen KT, Lund T, Jørgensen HB, Holdgaard PC, Ormstrup TE, et al. Baseline bone involvement in multiple myeloma - a prospective comparison of conventional X-ray, low-dose computed tomography, and 18 flourodeoxyglucose positron emission tomography in previously untreated patients. Haematologica 2016; 101(10):e415-8. doi: 10.3324/ haematol. 2016.146092.
- Tripathy S. The role of serum protein electrophoresis in the detection of multiple myeloma: an experience of a corporate hospital. J Clin Diagn Res 2012; 6(9):1458- 61.doi: 10.7860/ JCDR/2012/4213.2532.
- Liu Q. Diagnostic value of serum immunofixation elec-trophoresis and immunoglobulin quantification in multiple myeloma. Henan Med Res 2014; 23(11):50-2.
- Yan Z. Clinical study of immunofixation electrophoresis in the diagnosis and typing of multiple myeloma. China Modern Doctor 2016; 54(24):25-7.