Use of Bilateral Superficial Cervical Plexus Block for Excision of Thyroglossal Duct Cyst in an ASA III Patient
By Abdulhakim Sengel1, Evren Buyukfirat2, Ramazan Aslanparcas2Affiliations
doi: 10.29271/jcpsp.2022.12.1644Sir,
Surgery for thyroglossal duct cyst excision was planned for a 57-year, 67-kg, male patient using the bilateral superficial cervical plexus block (SCPB) method. The patient was a smoker and had heart failure (New York Heart Association (NYHA) Classification 3) and Grade 2 moderate dyspnea. The patient’s American Society of Anaesthesiology (ASA) risk score was evaluated as III. The patient was informed about the procedure to be performed and consent was obtained. After routine anaesthesia monitoring, premedication was performed with 2 mg Midazolam intravenously. Bilateral SCPB was planned for regional anaesthesia as described by Gürkan et al.1 Using the linear probe of ultrasound (US) (Toshiba, Nemio XG SSA-580A, Japan), the fascial area was reached after passing the skin, subcutaneous area, platysma muscle, sternocleidomastoid muscle, and superficial cervical fascia in plane (Figure 1A). After confirming that there was no intravascular access with negative pressure, 1 ml of local anaesthetic solution was administered first to confirm local anaesthetic distribution with US in the facial area, 7 ml of 0.5% bupivacaine and 5 ml of 2% lidocaine solution were injected bilaterally with intermittent negative aspirations, 12 ml for each region, a total of 24 ml. Block needle (Braun, Melsungen, Germany) with a 5 cm long, sonovisible, 22 G extension line was used for the SCPB (Figure 1A). After the success of the SCPB was confirmed with the pin-prick test and the loss of cold sense test, the surgical procedure (Figure 1B, 1C) was started, and no additional analgesic was given to the patient during the cyst excision (Figure 1C, 1D, 1E) lasting 40 minutes. The patient did not need analgesics for 24 hours postoperatively and was discharged without any complications.
The superficial cervical plexus (SCP) innervates the anterior and lateral region of the neck through the anterior branches of the 2nd and 4th cervical nerves, and by the block of this plexus, anaesthesia can be achieved at these regions of the neck.2 SCP is in an anatomically easy and accessible place.3 Unilateral SCPB can be preferred in cases such as submandibular mass excision and carotid endarterectomy. Bilateral SCPB is usually not preferred because of the risk of bilateral phrenic nerve paralysis that can cause respiratory arrest. In this case, we shared our experience of bilateral SCPB in a patient who underwent thyroglossal duct excision. US-guidance was not used in most of the blocks reported in the literature. It has been reported that US-guided blocks are both safer and require less local anaesthesia.1,3,4 Despite these advantages, complications may occur due to the involvement of the phrenic nerve, recurrent laryngeal nerve, and vagus, especially in bilateral SCPB. Phrenic nerve involvement can cause severe respiratory distress.5 In bilateral SCPB, keeping the drug dose low and using US can significantly reduce complications. To avoid these, we kept drug doses low for both sides. Necessary preparations were made considering the possibility of general anaesthesia. SCPB may prove useful in providing both anaesthesia and analgesia in patients with high anaesthesia risk.
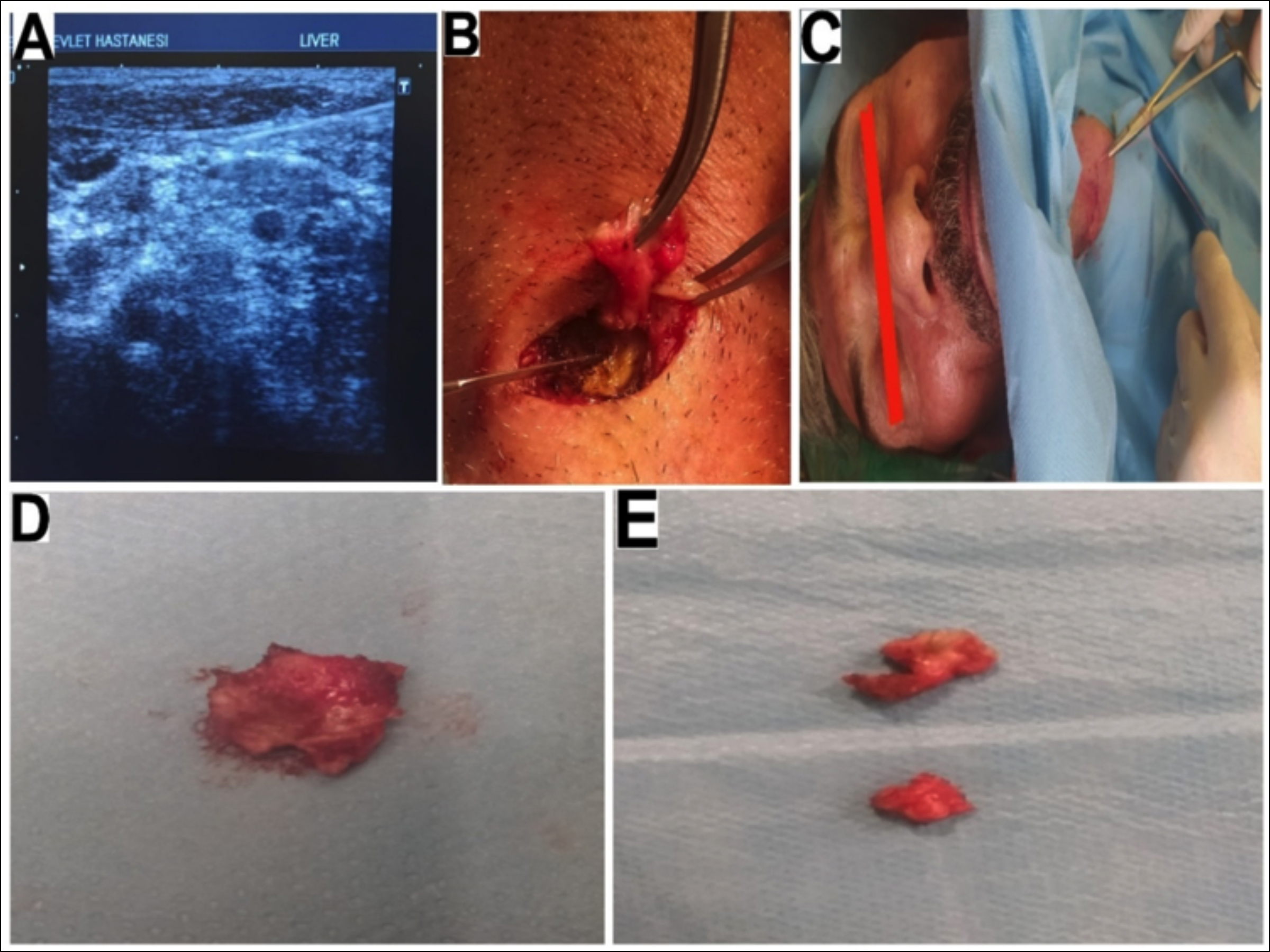 Figure 1: (A) Ultrasound image of SCPB. (B) In-operation image. (C) End of operation image. (D, E) Thyroglossal duct cyst tissues were removed in the operation.
Figure 1: (A) Ultrasound image of SCPB. (B) In-operation image. (C) End of operation image. (D, E) Thyroglossal duct cyst tissues were removed in the operation.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
AS: Concept, supervision, and data collection.
EB: Design, critical review, and interpretation.
RA: Literature review, writing the article, references, and funding.
All the authors have approved the final version of the manuscript to be published.
REFERENCES
- Gürkan Y, Taş Z, Toker K, Solak M. Ultrasound guided bilateral cervical plexus block reduces postoperative opioid consumption following thyroid surgery. J Clin Monit Comput 2015; 29(5):579-84. doi: 10.1007/ s10877-014-9635-x.
- Standing S, Borley NR, Collins P, editors. Gray’s Anatomy: The anatomical basis of clinical practice. 40th ed. London, UK: Churchill Livingstone Elsevier; 2008.
- Gürkan Y, Kuş A, Aksu C, Ohtaroğlu C, Solak M, Toker K. Changing trends and regional anesthesia practices in Turkey. Agri 2014; 26(3):131-7. doi: 10.5505/agri.2014. 26056.
- Mukhopadhyay S, Niyogi M, Dutta M, Ray R, Gayen GC, Mukherjee M, et al. Bilateral superficial cervical plexus block with or without low-dose intravenous ketamine analgesia: Effective, simple, safe, and cheap alternative to conventional general anesthesia for selected neck surgeries. Local Reg Anesth 2012; 5:1-7. doi: 10.2147/ LRA.S28360
- Erdine S. Head and neck related blocks. In: Regional anesthesia.1st Edition, Istanbul, Nobel Medicine Bookstores 2005; 76-8.