Urachal Actinomycosis Presenting with Recurrent Urinary Tract Infections in a Middle-aged Woman: A Rare Case Report
By Basri Cakiroglu1, Cevdet Kaya2, Suleyman Hilmi Aksoy3, Ramazan Gozukucuk4, Lora Ates5Affiliations
doi: 10.29271/jcpsp.2022.05.668ABSTRACT
The urachal cyst, a remnant of allantois sac during embryogenesis, is a rare condition in adulthood. Urachus is an embryologic remnant degenerating after birth. Abberrant obliteration of the urachus causes urachal abnormalities. The urachal cysts are almost always symptomatic when infected. The symptoms include fever, abdominal pain, tenderness, lower abdominal mass, nausea, vomiting, and dysuria. Ultrasonography, computerised tomography, and magnetic resonance imaging techniques may be insufficient for diagnosis. In most cases, staphylococcus species are isolated from cultures of urachal cysts. Other microorganisms such as Escherichia coli, Enterococcus faecium, Klebsiella pneumonia, and rarely actinomyces may be isolated.
Actinomyces, an anaerobic gram-positive filamentous bacterium, is a rare cause of granulomatous disease. In this case report, a 56-year woman with urachal cyst infection with actinomyces is discussed according to current knowledge.
Key Words: Urachal cyst, Urachus, Chronic cystitis, Actinomyces.
INTRODUCTION
The urachus is an embryologic remnant between the umbilicus and bladder, which degenerates after birth. The associated anomalies originating from urachus are rare. Of these, the infected urachal cysts cause clinical symptoms such as lower abdominal or suprapubic pain, fever, urination problems, and a suprapubic palpable mass. Complications of infected urachal cysts include: drainage into the bladder or umbilicus, peritonitis by peritoneal drainage, extraperitoneal rupture, recurrent urinary tract infections, intestinal fistulas, ureter obstruction, and late urachal adenocarcinoma.1,2
Actinomycosis is a progressive chronic suppurative inflammatory disease, which is characterised by heavy granulation tissue formation and may result in abscess and fistula formation.3 The disease generally spreads to neighboring organs. Actinomycosis does not spread via lymphatics and lymphadenopathy is not an important finding in these cases.
The hematogenous spread is also rare. Although it can infect all intraabdominal organs, it commonly occurs at the ileocecal region, especially involving the caecum and appendix, which are stagnant regions of the gastrointestinal tract. Actinomyces infection of urachal cyst is very rare.
In this case report, a 56-year woman with urachal cyst infection with actinomyces is discussed.
CASE REPORT
A 56-year woman was admitted to the hospital with complaints of dysuria and lower abdominal pain. The patient had a history of lower urinary tract infection (UTI) treated with antibiotics according to the antibiogram. The patient had relapsing UTI four times and underwent ultrasonography, which revealed a heterogeneous lobulated solid mass of 110×75 mm, at the superior aspect of the bladder. In the physical examination, a solid mass beginning from the umbilicus to the suprapubic area was palpated on both sides of the midline, fixed to the rectus abdominis muscle. The chest x-ray was normal. Laboratory tests for both kidney and liver function tests were normal. Complete blood count showed severe leukocytosis and mild anemia (white blood cells, 26.10×103/μL (Normal: 4.16-10.2×103/μL). Haematocrit was 34.7% (Normal: 36-47%), and hemoglobin was 11.4 g/dL (Normal: 12-16 g/dL)). Abdominal MR imaging showed a solitary lesion composed of the mostly necrotic papillary lesions with peripheral oedema and inflammation. The mass, measuring 11.5 × 10.5 mm, was located from the bladder dome to the umbilicus and extended to the left side of the midline (Figures 1 and 2).
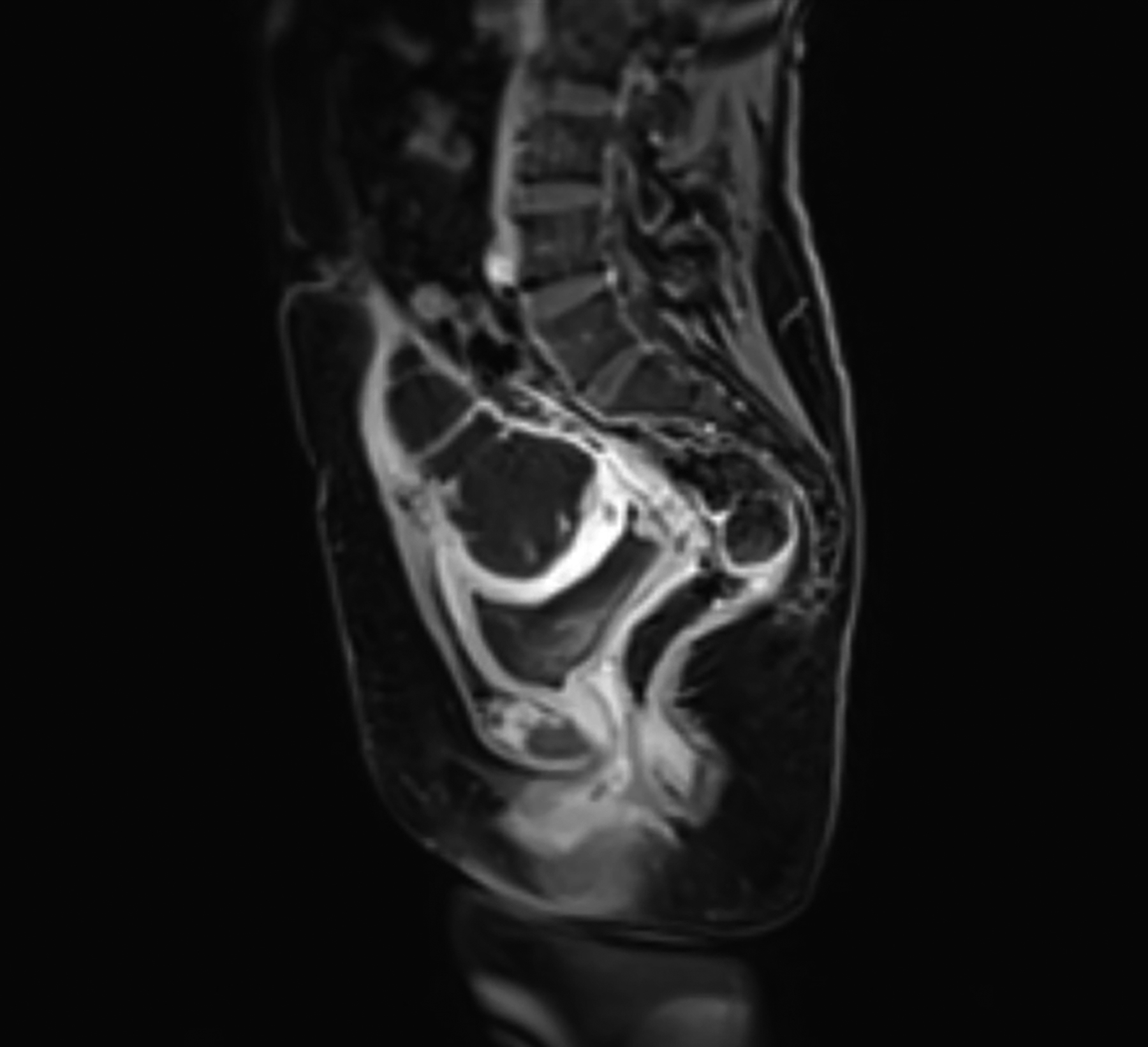 Figure 1: T1-weighted sagittal image of magnetic resonance imaging showed an urachal abscess.
Figure 1: T1-weighted sagittal image of magnetic resonance imaging showed an urachal abscess.
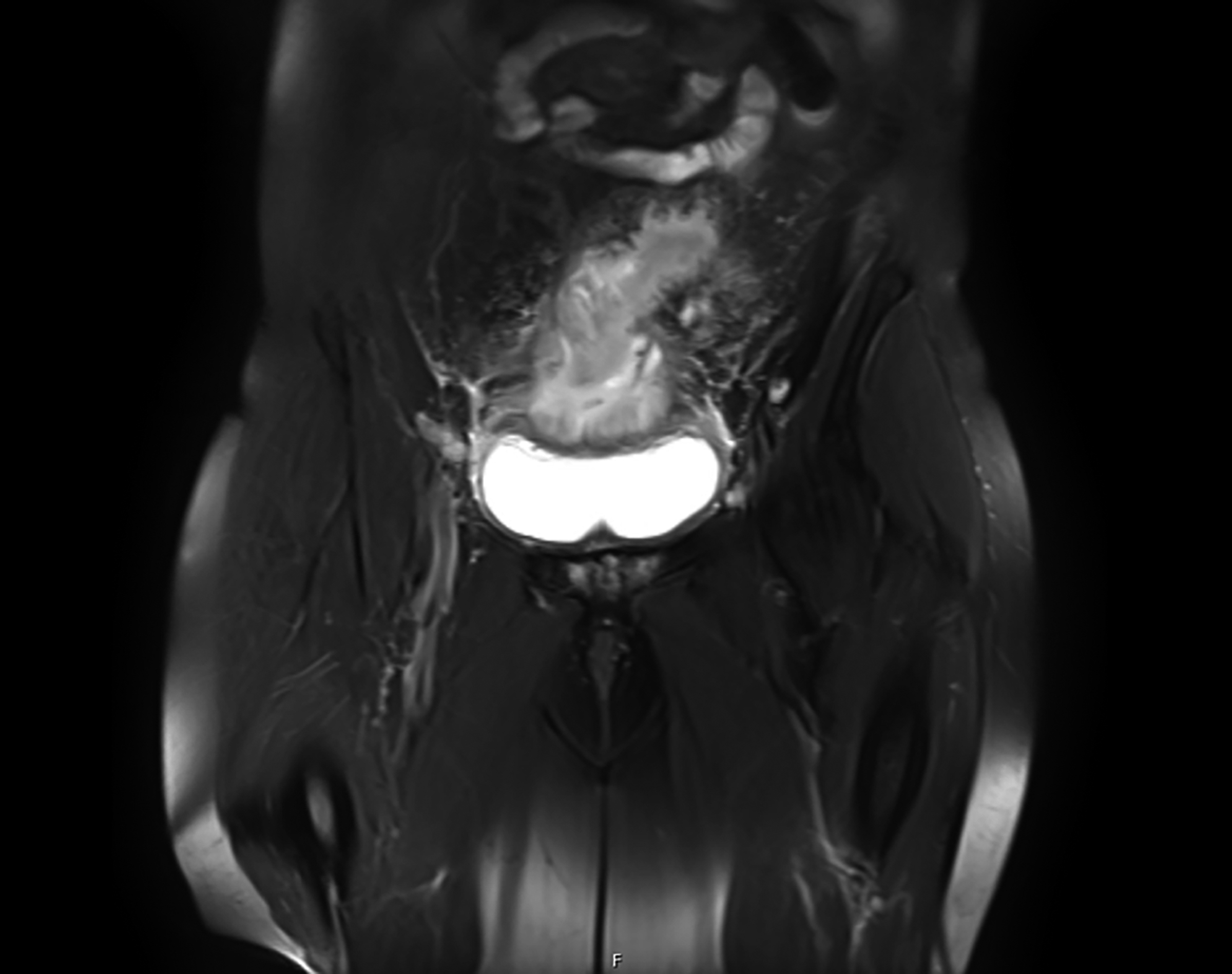 Figure 2: Preoperative lower abdominal MR images.
Figure 2: Preoperative lower abdominal MR images.
A cystoscopic examination was performed before the surgical operation to rule out malignancy. A biopsy was taken and histopathological examination was consistent with chronic cystitis.
According to all above findings, the patient was diagnosed as a urachal cyst and underwent the operation. The urachal cyst excision with partial cystectomy was performed. The pathological examination showed intense mixed inflammatory cell infiltration including polymorphonuclear leukocytes, lymphocytes, plasma cells, and histiocytes. The microscopic examination also revealed fibrosis, oedema, chronic inflammation, lymphoid follicle formations, actinomyces colonies, and vascular proliferation and ectasia at the periphery. Additionally, erosion was demonstrated in the bladder epithelium (Figure 3). No malignancy was detected.
The patient was administered oral amoxicillin treatment for 8 weeks postoperatively. In the second month of follow-up, the patient's wound was completely healed. Her symptoms resolved, and anaemia and leukocytosis improved. In the 8th month, the patient had swelling and pain in the incisional region. The ultrasonography and MRI showed a hernia, and no recurrence of the disease. The incisional hernia was repaired laparoscopically.
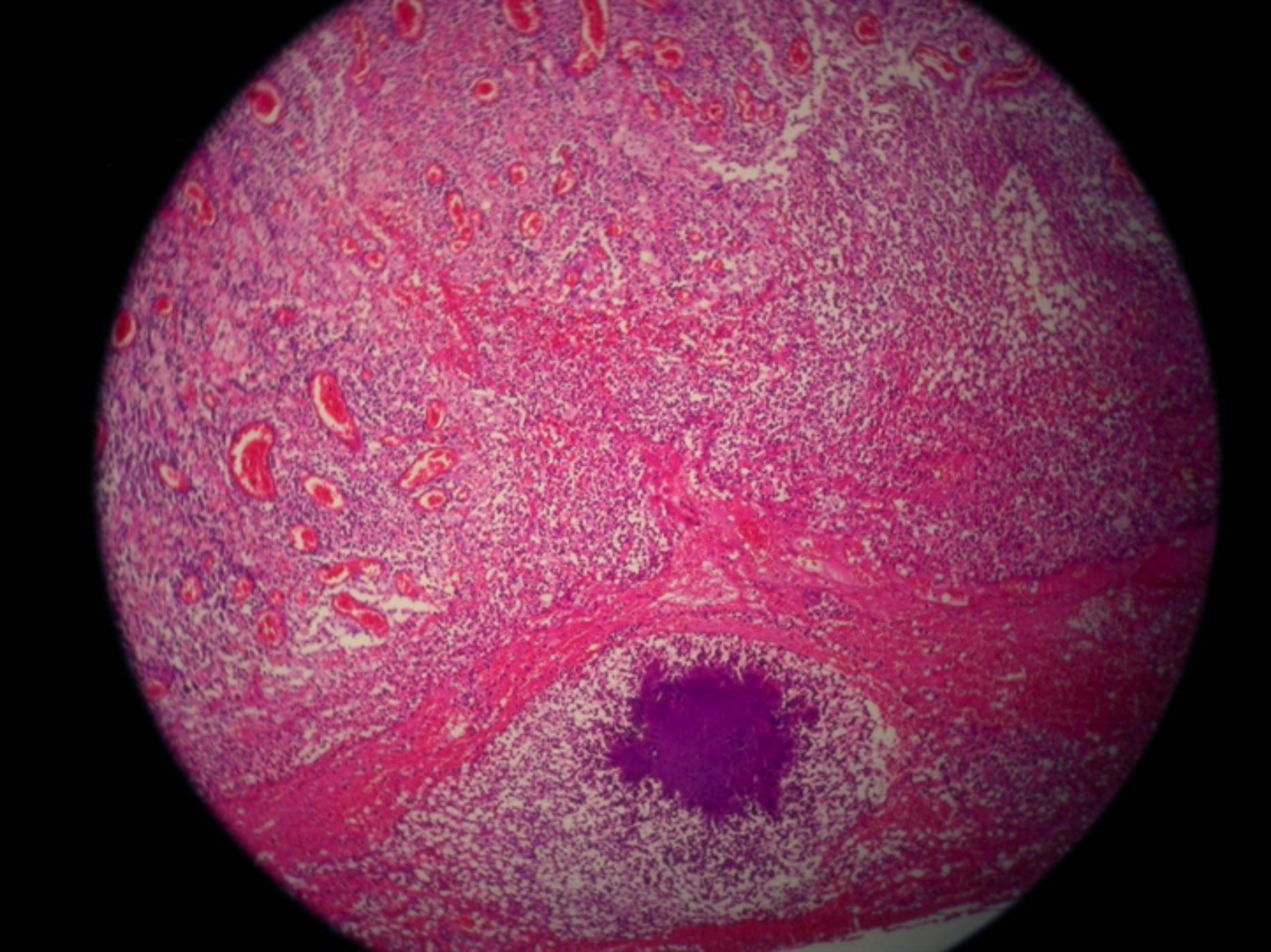 Figure 3: Sulphur granules of actinomyces with peripheral mixed ınflammatory reaction. H&E staining, 100x.
Figure 3: Sulphur granules of actinomyces with peripheral mixed ınflammatory reaction. H&E staining, 100x.
DISCUSSION
The urachus is a fibrous remnant of allantois which regresses progressively after birth and extends from the umbilicus to the dome of the bladder.4 Incomplete obliteration of the urachal canal causes various anomalies including the patent urachus, urachal sinus, vesicourachal diverticula and urachal cysts. A urachal cyst occurs in the remnant between the umbilicus and bladder.5 The urachal cysts become symptomatic when infected, and cause fever, abdominal pain, abdominal tenderness, lower abdominal mass, nausea, vomiting, and dysuria.6
The patient in this case had recurrent UTIs and dysuria. In physical examination, there was lower abdominal mass and stiffness.
In cultures, generally staphylococcus species are isolated. Other microorganisms such as Escherichia coli, Enterococcus faecium and Klebsiella pneumonia can also be seen.7,8 The most pathogenic type of actinomyces is A. israelii, an anaerobic gram-positive filamentous bacteria and a rare cause of chronic granulomatous disease. Actinomycosis is a chronic and recurrent disease that affects all urogenital organs, including the kidneys and bladder.3,8
The infection of urachus with actinomycosis is rarely reported and the patients with such a condition usually report mass symptoms below the umbilicus, abdominal pain, weight loss, loss of appetite, fever, and laboratory signs of leukocytosis and anaemia.9 Recurrent UTIs should be evaluated further in case an underlying etiological cause may be revealed before continuing antibiotics. In this case, a urachal cyst were detected in the ultrasonographic examination after recurrent UTIs. E.coli was isolated in urine culture. There was no fever or weight loss, but she had fatigue. Leukocytosis and anaemia were determined in the laboratory examination. Fistula contents or tissue biopsy samples taken from lesions are usually examined for the diagnosis of actinomycosis. However, it is difficult to identify actinomyces in samples because of other filamentous and anaerobic bacteria. For this reason, the diagnosis cannot be made at the time of the evaluation of the patient.10 The definitive diagnosis of our patient was made after the pathological examination of the specimen.
The drainage of the abscess is not advised due to the high risk of recurrence and malignancy. We preferred open surgery in this case because our patient's mass was very large and attached to the skin.
Since the clinical and the radiological findings are not specific for actinomycosis, in most cases, the diagnosis can be made only after surgery, as in this case. The recent literature states that it is difficult to differentiate actinomycotic masses from malignant tumors prior to surgical excision. The cystoscopic examination is recommended to rule out malignancy before surgical operation. Surgical intervention is useful for debridement of necrotic tissues, removal of persistent sinuses, and definitive diagnosis. Actinomycosis is treated with surgery and antibiotics.1-5 For two weeks, intravenous penicillin should be given. Treatment should continue for 6-12 months. In case of penicillin allergy, tetracycline, erythromycin, and ciprofloxacin can be used.3-10 After the operation, we extended the course of oral amoxicillin therapy for 8 weeks.
This case highlights the need to keep actinomycosis in the differential diagnosis of urachal cyst anomalies presenting with mass-like features.
PATIENT'S CONSENT:
Patient's permission was obtained to publish the case report.
COMPETING INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
BC, CK, SHA, LA: Involved in the case, gathered data, drafted the report and final approval, agreed to be accountable for parts of the work.
REFERENCES
- Yu JS, Kim KW, Lee HJ, Lee YJ, Yoon CS, Kim MJ. Urachal remnant diseases spectrum of CT and US findings. Radiographics 2001; 21(2):451-61. doi: 10.1148/radio graphics.21.2.g01mr02451.
- Numanoglu V, Sogut A. A rare cause of recurrent urinary system infections: Urachus cyst. Turk Arch Pediatr 2004; 39(4):181-4.
- Çakıroglu, B, Gozukucuk R, Aksoy SH, Guclu M, Ates L. Renal kolik ile giden ilginc bir aktinomikoz olgusu. Abant Tip Dergisi 2013; 2(3): 245-7.
- Ashley RA, Inman BA, Routh JC, Rohlinger AL, Husman DA, Kramer SA. Urachal anomalies: A longitudinal study of urachal remnants in children and adults. J Urol 2007; 178:1615-6. doi:10.1016/j.juro.2007.03.194.
- Berman SM, Tolia BM, Laor E, Reid RE, Schweizerhof SP, Freed SZ. Urachal remnants in adults. Urology 1988; 31(1):17-21. doi: 10.1016/0090-4295(88)90564-X.
- Allen JW, Song J, Velcek FT. Acute presentation of infected urachal cysts: Case report and review of diagnosis and therapeutic interventions. Pediatr Emerg Care 2004; 20(2):108-11. doi: 10.1097/01.pec.0000113880.10140.19.
- MacNeily AE, Koleilat N, Kiruluta HG, Homsy YL. Urachal abscesses: Protean manifestations, their recognition, and management. Urology 1992; 40(6):530-35. doi: 10.1016/ 0090-4295(92)90409-p.
- Maddah G, Feizzdeh Kerigh B, Mohamadian N, Bagheri V. Primary urachal actinomycosis: Case report and literature review. Nephrourol Mon 2013; 5(5):997-1000. doi:10. 5812/numonthly.10933.
- Singh A, Prasad HK, Shetty KJ, Philip NR, Salma R, Chakravarthy A. Urachal cyst with xanthogranulomatous cystitis: A rare case report. Urol Ann 2018; 10(2):219-21. doi: 10.4103/0974-7796.229555.
- Yeung VH, Wong QH, Chao NS, Leung MW, Kwok WK. Thoracic actinomycosis in an adolescent mimicking chest wall tumor or pulmonary tuberculosis. Pediatr Surg Int 2008; 24(6):751-4. doi: 10.1007/s00383-008-2155-3.