Robinow Syndrome: A Rare Diagnosis from Pakistan
By Marya Hameed, Syed Maaz Tariq, Hina HanifAffiliations
doi: 10.29271/jcpsp.2023.01.120Sir,
Robinow syndrome is an extremely rare syndrome of mesomelic dwarfism.1 It is characterised by short stature, dysmorphic head, face, and external genitalia abnormalities. Due to the classic resemblance to fetal face with laterally displaced eyes, pointed nasal ala, and frontal head prominence, it is also known as “fetal facies syndrome”.2 There is a geographical predilection for the Middle East, South Asia and some parts of Europe. The diagnosis is typically considered easier owing to the characteristic pattern of physical manifestations.1,2
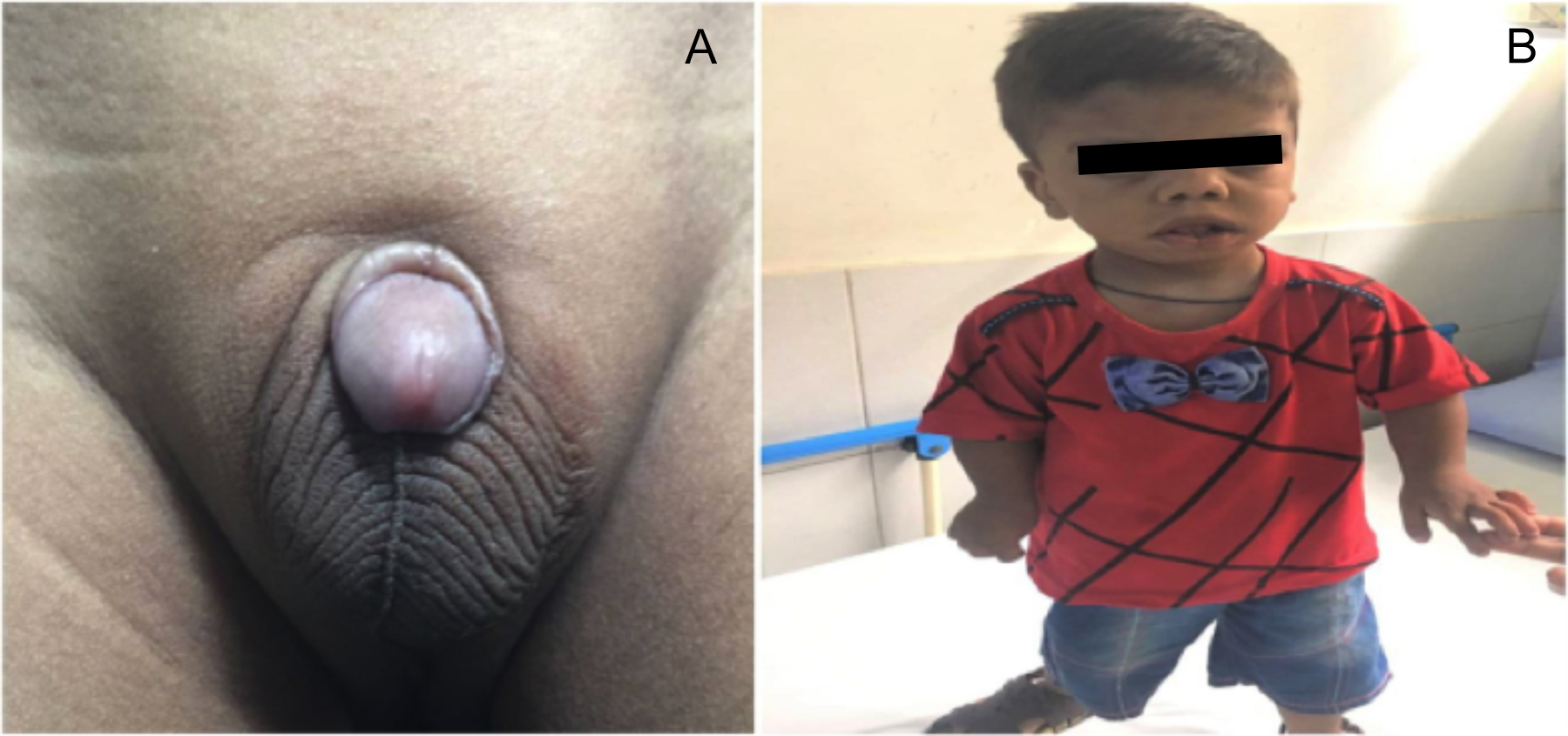 Figure 1: Physical anomalies. A. Micropenis, B. Dysmorphic facies with frontal bossing, hypertelorism anteverted nostrils, long philtrum and short stature.
Figure 1: Physical anomalies. A. Micropenis, B. Dysmorphic facies with frontal bossing, hypertelorism anteverted nostrils, long philtrum and short stature.
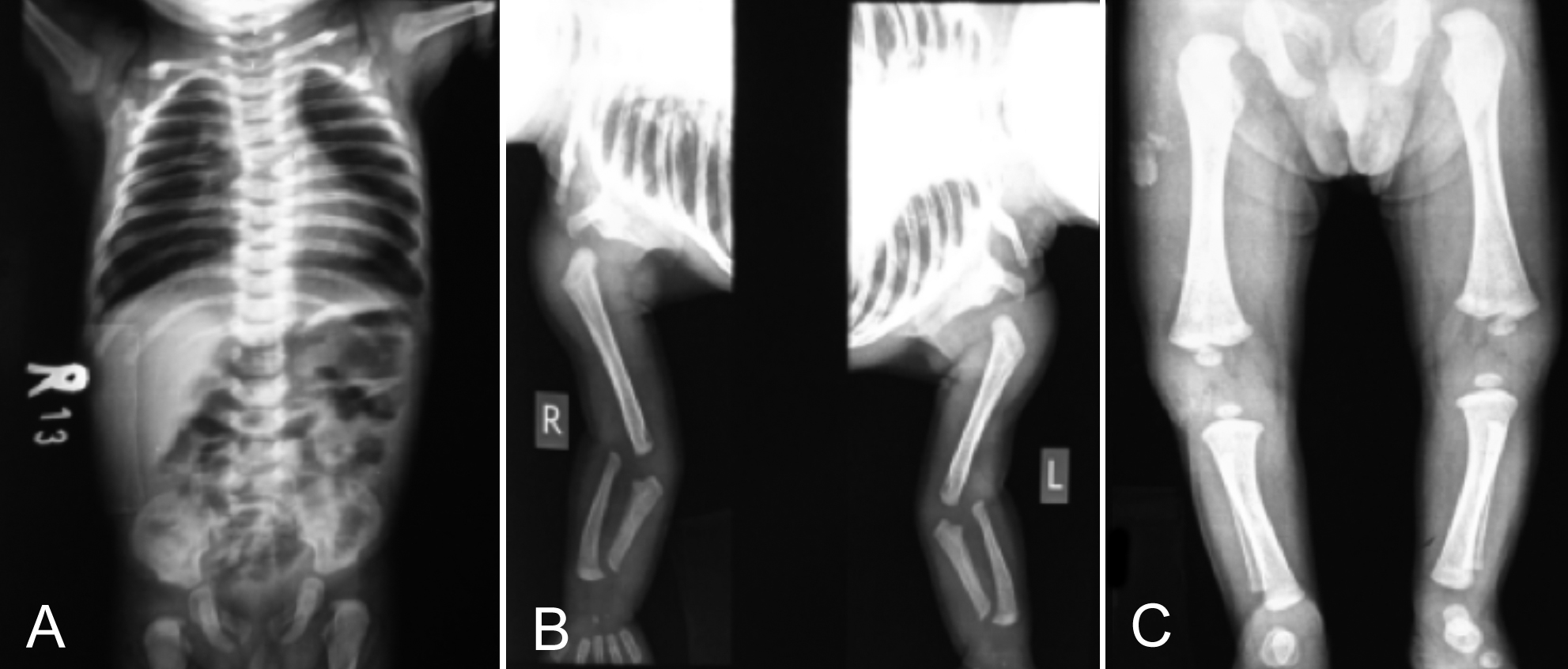 Figure 2: A D5 Hemivertebra resulting in slight angulation towards the right side. B and C. Mesomelia of upper and lower extremities.
Figure 2: A D5 Hemivertebra resulting in slight angulation towards the right side. B and C. Mesomelia of upper and lower extremities.
A 3-year boy was reported to the outpatient department with a complaint of short stature. His parents were unrelated and his mother underwent a normal pregnancy. The prenatal period was insignificant and the family history of both parents was negative for any genetic and birth defects. The anthropometric measurements were as follows: height, 80 cm; weight, 10 kg; fronto-occipital circumference, 53cm; arm span, 69cm and arm span/ height ratio, 0.884; upper segment, 49cm; lower segment, 32cm and upper to lower segment ratio, 1.53. Examination was significant for macrocephaly, frontal bossing, hypertelorism, downward slanting of the right eye, depressed nasal bridge, anteverted nostrils, micrognathia and inverted V upper lip (Figure 1). All four limbs were short compared to the trunk but with normal toes and fingers. Genital examination was significant for micro-penis (length, 2 cm) which was buried under the surrounding skin; scrotum was rugated and well formed (Figure 1). The skeletal survey revealed straightening of normal kyphotic curvature of dorsal spine with D5 hemivertebra resulting in angulation towards the right side and crowding of 5th and 6th right ribs (Figure 2). Mesomelic shortening was noted and hand radiographs were significant for clinodactyly. Ultrasonography of scrotum revealed a right undescended testis. The physical and radiological findings were collectively indicative of Robinow syndrome.
A syndrome of mesomelic shortening of limbs, hemivertebra, and hypoplasia of the genitalia was first described by Robinow in 1969. The exact incidence of Robinow syndrome is poorly documented and there is no gender predilection. Autosomal recessive form of the disease has been reported from Oman due to high rates of consanguineous marriages. High frequency has also been observed in Turkey.3
Dominant and recessive forms share a number of characteristics such as facial features, gingival hypertrophy, orodental abnormalities, maldeveloped genitalia, hypoplasia of midface, upturned nose with nasal bridge shortening, frontal bossing, and upper lip tenting, which resembles an inverted ‘‘V’’. In the oral cavity, due to the presence of both primary and secondary sets of teeth, malocclusion and overcrowding occurs with incisors exposure secondary to an upper lip tenting. Tongue-tie (ankyloglossia) and bifid tongue are also reported to be associated.4
Prenatal diagnosis may be offered at 19 weeks with the aid of fetal ultrasound. Treatment with human chorionic gonadotropin (hCG) is helpful to increase penile length and also has favourable effects on the growth of patients.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
MH, SMT, HH: Drafting, editing, and final approval.
REFERENCES
- Suresh S. Robinow syndrome. Indian J Orthop 2008; 42(4):474-6. doi: 10.4103/0019-5413.43399.
- Mishra S, Agarwalla SK, Pradhan S. Robinow syndrome: A Rare Diagnosis. J Clin Diagn Res 2015; 9(12):Sd04-5. doi: 10.7860/JCDR/2015/15078.6949.
- Akşit S, Aydinlioglu H, Dizdarer G, Caglayan S, Bektaşlar D, Cin A. Is the frequency of Robinow syndrome relatively high in Turkey? Four more case reports. Clin Genet 1997; 52(4):226-30. doi: 10.1111/j.1399-0004.1997.tb02552.x.
- Saraswat S, Mohanty S. Robinow syndrome: A rare case report from a tertiary care Hospital in Eastern India. J Int J Pediatr 2016; 4(10):3643-9.