Non-Surgical Management of Lingual Hemangioma by Combined Sclerotherapy and Cryotherapy
By Shaul Hameed Kolarkodi1, Muhammad Qasim Javed2, Mohammed Rafeeq PK3, Dhafer Alasmari4, Mohammed Faiz CP5Affiliations
doi: 10.29271/jcpsp.2022.08.1080ABSTRACT
Hemangioma is frequently seen benign tumour of vascular origin, typed into capillary and cavernous hemangiomas based on the nature of vessels in the lesions. Capillary hemangioma is a collection of small capillary-size vessels and shows lobule formation. Cavernous hemangioma is formed by the large dilated vessels and it can reach a large size. The hemangioma can cause aesthetic and functional problems when it is located on the tongue. Several treatment modalities including sclerotherapy, embolisation, laser surgery, and cryosurgery have been described. Here, we are reporting a case of a 12-year boy diagnosed with a hemangioma on the left lateral border of the tongue using ultrasonography with color Doppler application and treated non-surgically with sclerotherapy and cryotherapy.
Key Words: Color Doppler ultrasonography, Cryotherapy, Hemangioma, Sclerotherapy, tongue.
INTRODUCTION
The term vascular lesions include conditions resulting from the abnormal position, structure, or number of the blood vessels.1 Classification by the International Society for the Study of Vascular Anomalies has differentiated between the two major types of vascular aberrations; vascular malformations and vascular tumours.2 Vascular tumours are differentiated from the vascular malformations by their clinical appearance, radiological characteristics, pathological features, and biological behavior.3 Vascular malformations stem from quiescent endothelium. Conversely, vascular tumours like hemangioma are the result of the benign proliferation of endothelial cells of vascular origin and relatively rare on the tongue. Hemangiomas are divided into either capillary or cavernous types.4 Capillary hemangioma is formed by small capillary-size vessels that organize in a lobular form. On the other hand, cavernous hemangioma is comprised of dilated, large vessels, and can reach a large-size.
The treatment modality for hemangioma depends upon the age/general condition of the patient and the size/characteristics of the lesion. Lesions of smaller size can be surgically excised while larger ones need non-surgical interventions like sclerotherapy, embolisation, laser surgery, and cryosurgery.5
The current report describes the case of a 12-year boy with hemangioma of the tongue diagnosed by using color Doppler ultrasonography and successfully treated with sclerotherapy and cryotherapy.
CASE REPORT
A 12-year boy presented to the Department of Oral Medicine and Radiology for the management of swelling at the lateral aspect of the tongue on the left side. The swelling was small in size initially and increased in size gradually over the past three years. There was no history of any associated symptoms or bleeding/discharge from the swelling. The medical history of the patient was unremarkable. The extraoral examination did not show any facial asymmetry or swelling. Moreover, no lymph nodes were palpable. The intraoral examination revealed solitary dome-shaped swelling present on the middle one-third of the left lateral border of the tongue with bluish-purple color (Figure 1A). It was 3×2 cm in dimensions with well-defined borders. The swelling surface appeared to have normal papillations. There was no limitation of tongue movement. On palpation, it was painless, fluctuant, non-reducible, and compressible with no pulsatility. On the chair-side diascopy test, blanching was noted.
 Figure 1: (a) Deep bluish-colored dome-shaped lesion on the left lateral border of the tongue, and (b) Post-treatment image showing complete regression of the lesion at the one-month follow-up.
Figure 1: (a) Deep bluish-colored dome-shaped lesion on the left lateral border of the tongue, and (b) Post-treatment image showing complete regression of the lesion at the one-month follow-up.
Based on the clinical examination and chair-side investigation, a provisional diagnosis of hemangioma of the tongue was made. Subsequently, to confirm the diagnosis ultrasonography (USG) of the swelling was done with the color Doppler application. USG showed multiple hypoechoic areas with no evidence of calcification within the lesion thus, confirming the diagnosis of hemangioma (Figure 2a). On color Doppler application, it presented diffuse vascular signals within the lesion suggestive of arteriovenous malformation which means capillary as well as cavernous structure (Figure 2b). Parents were informed about the diagnosis, treatment options, risks, prognosis, and consent was taken. Later, the patient was treated with two cycles of intralesional sodium tetradecyl sulfate injection and cryotherapy using liquid nitrogen at an interval of two weeks. The lesion showed complete regression without any complication for four weeks after the second cycle. Tongue movements were normal and there was no change in speech and taste sensation (Figure 1b).
DISCUSSION
Vascular tumours like hemangiomas are soft tissue tumours that either present congenitally or manifest themselves later. They rarely occur in the tongue. In the case presented here, the patient had a hemangioma on the left lateral side of the tongue. Depending on the type of vascular tumours, they can either persist or regress on their own. Conversely, vascular malformations usually persist during the whole life.2 The management of vascular lesions depends upon many factors including their type. In the past, clinical and histological examinations of the lesion were the cornerstones of the diagnosis. However, recently imaging approaches particularly, ultrasound has demonstrated its utility for diagnosing oral cavity diseases.1 Therefore, in the current case report, USG was used with color Doppler application for the diagnosis.
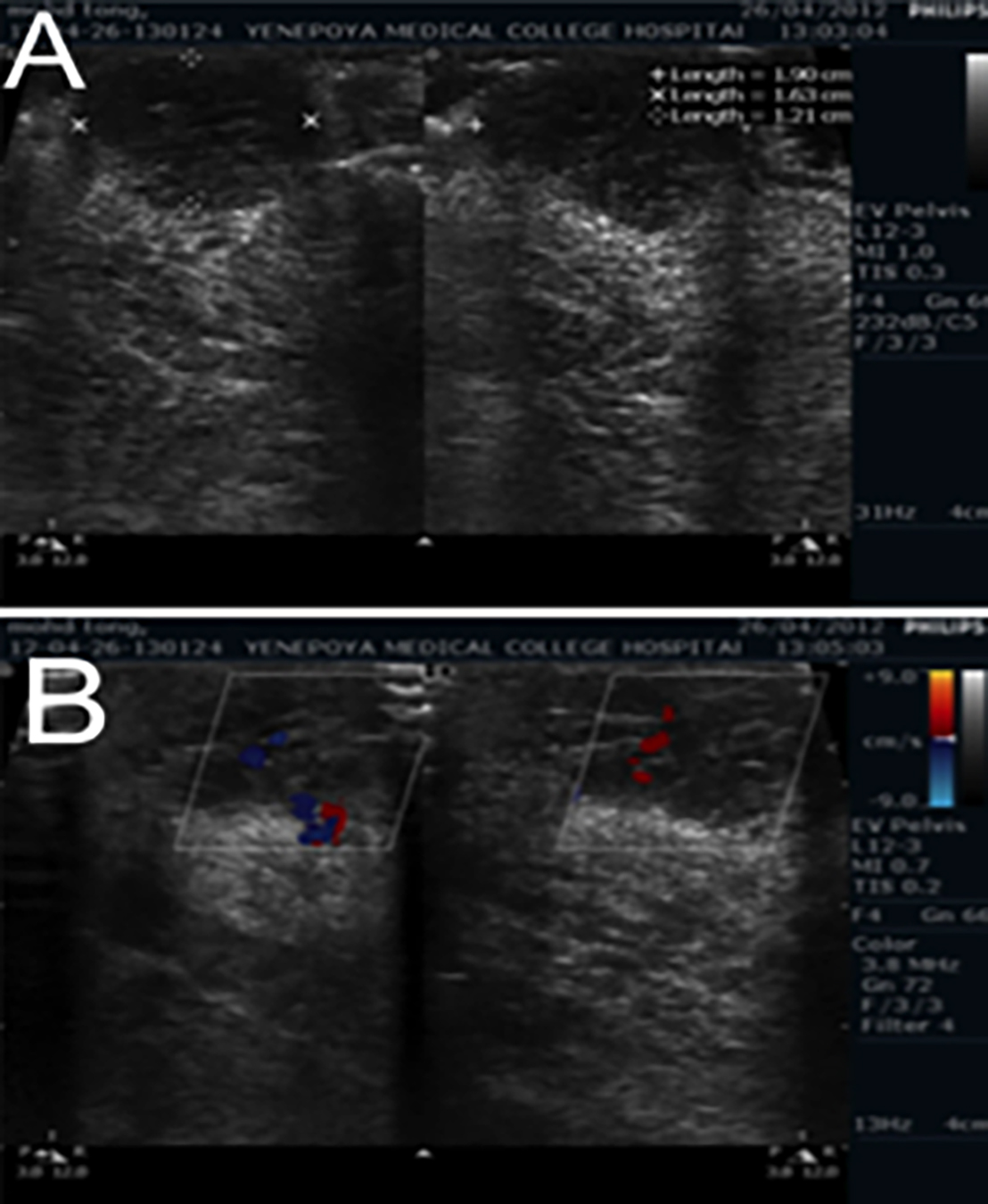 Figure 2: (a) Ultrasonographic image with hypoechoic areas with no evidence of calcification, and (b) Color Doppler application depicting areas in blue and red indicating hemangioma.
Figure 2: (a) Ultrasonographic image with hypoechoic areas with no evidence of calcification, and (b) Color Doppler application depicting areas in blue and red indicating hemangioma.
The tongue hemangiomas require special attention because of their susceptibility to trauma that can lead to bleeding, ulceration, swallowing/breathing difficulties, and cosmetic issues.6 Multiple management strategies for treating hemangiomas have been documented that include primary surgical excision, electrolysis, embolisation, steroid injection, laser photocoagulation, cryotherapy, sclerotherapy, and combined sclerotherapy/cryotherapy.1 Although excision is effective, yet it is not widely utilised because of the possible risk of bleeding and scarring. On the other hand, sclerotherapy has been adopted in the wide number of cases because of its efficiency in limiting the damage to the tissues surrounding the lesion.7 This method involves the injection of a sclerotic agent into the peripheral vein from where the hemangioma originates. This method is superior in treating extraoral lesions as the application of pressured bandage could not be attained inside the oral cavity in case of intraoral lesions. Therefore, sclerotherapy combined with other modalities like cryotherapy is recommended. Hence, in our case sclerotherapy was augmented with cryotherapy.
The main principle of cryosurgery is cold-induced coagulative necrosis of the benign neoplastic tissue that usually requires the attainment of a minimal −15°C temperature.4 For the management of oral hemangioma, liquid nitrogen, delivered through probes/sprays, is used as a coagulating agent.5 In the current case, a probe was utilised for the delivery because of its limited targeted effect on the lesion. Also, the application of cryosurgery aids in the faster regeneration and minimal amount of nerve damage with lesser scar formation.8
In conclusion, sclerotherapy combined with cryotherapy is a viable management option for vascular tumours like hemangioma on the tongue. In the current case, injection of sclerosing agent followed by the application of cryotherapy resulted in the faster and complete regression of the lesion hence, we were successful in accomplishing the patient’s aesthetic recovery by the non-surgical method.
PATIENT’S CONSENT:
Informed consent was taken from the patient’s family for the publication of his images.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
SHK: Diagnosis of lesion, preoperative preparation of the patient, and acquisition of data.
MQJ: Design, write-up, and critical appraisal of the work.
MR: Operative procedure and concept.
DA: Final review of the manuscript.
MFCP: Literature review and editing.
All the authors have approved the final version of the manuscript to be published.
REFERENCES
- Gianfranco G, Eloisa F, Vito C, Raffaele G, Gianluca T, Umberto R. Color-doppler ultrasound in the diagnosis of oral vascular anomalies. N Am J Med Sci 2014; 6(1):1-5. doi: 10.4103/1947-2714.125852.
- Enjolras O, Mulliken JB. Vascular tumours and vascular malformations (new issues). Adv Dermatol 1997; 13: 375- 423.
- Wassef M, Enjolras O. Superficial vascular malformations: Classification and histopathology. Ann Pathol 1999; 19(3): 253-64.
- Langdon JD, Patel MF. Operative maxillofacial surgery. London: Chapman and Hall Medical; 1998. p.393-6.
- Tal H. Cryosurgical treatment of hemangiomas of the lip. Oral Surg Oral Med Oral Pathol 1992; 73(6):650-4. doi: 10.1016/0030-4220(92)90002-8.
- Chang CJ, Fisher DM, Chen YR. Intralesional photo-coagulation of vascular anomalies of the tongue. Br J Plast Surg 1999; 52(3):178-81. doi: 10.1054/bjps.1998.3056.
- Bonet-Coloma C, Mínguez-Martinez I, Palma-Carrio C, Galán-Gil S, Peñarrocha-Diago M, Mínguez-Sanz JM, et al. Clinical characteristics, treatment and outcome of 28 oral haemangiomas in pediatric patients. Med Oral Patol Oral Cir Bucal 2011; 16(1):19-22. doi: 10.4317/medoral.16.e19.
- Van Aalst JA, Bhuller A, Sadove AM. Pediatric vascular lesions. J Craniofac Surg 2003; 14(4):566-83. doi: 10.1097/ 00001665-200307000-00032.