Langerhans Cell Histiocytosis with an Undetected Ileal Polyp
By Mevlut Kiyak1, Alpaslan Tanoglu1, Dilek Yilmaz2Affiliations
doi: 10.29271/jcpsp.2022.08.1094Sir,
Langerhans cell histiocytosis (LCH) is a rare disease caused by the accumulation of dendritic cells in various organs similar to Langerhans cells in the epidermis. It has a clinical picture ranging from an accidental lesion to a serious disease that causes death. The most common systems affected by LCH are bones and skin.1 Gastrointestinal tract (GIT) involvement is extremely rare. In GIT, the disease is mostly seen in the stomach and rectum.2 To our knowledge, LCH presenting as an ileal polyp has not been previously reported.
A 60-year male was referred to our gastroenterology outpatient clinic due to iron deficiency anemia. Upper gastrointestinal endoscopy did not reveal anything pathological to explain iron deficiency anemia. No pathological lesion was observed in the colon during colonoscopy. However, there was a 15 mm pedunculated polyp in the terminal ileum and polypectomy was performed.
The polyp pathology was reported as LCH. Histopathology showed histiocytes forming large aggregates in the lamina propria of the mucosa. On immunohistochemistry, the cells were positive for CD-1a, S-100 protein, CD3, and CD68 (Figure 1).
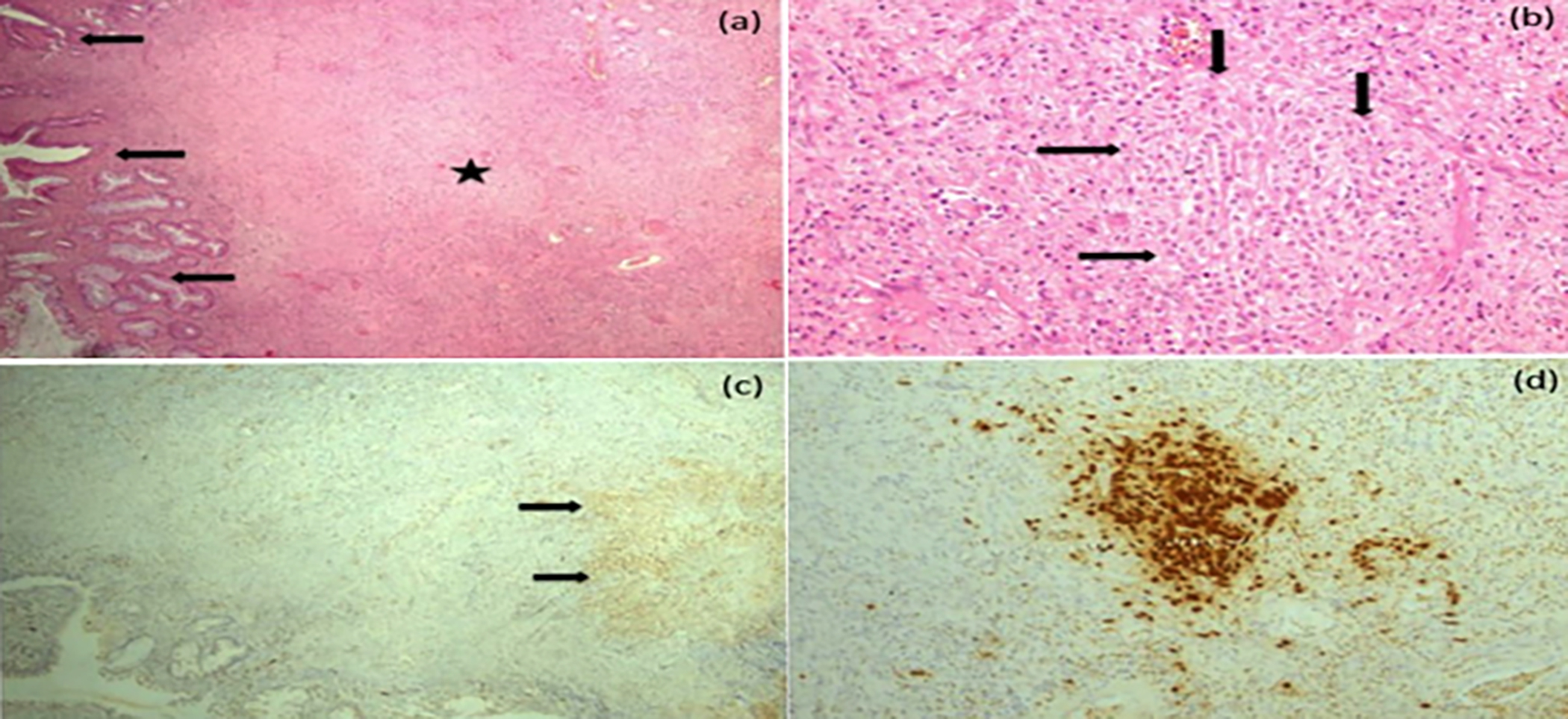 Figure 1: Histopathological and immunohistochemical features of the disease.
Figure 1: Histopathological and immunohistochemical features of the disease.
(a) Fibrotic and inflamed polypoid lesion with stroma (star) containing hyperplastic crypts (arrow) on the surface (b) Chronic active inflammation in the stroma as well as histiocytic cells forming irregular nodular collections (arrow) (H&E, ×100) (c) Collection of S-100 positive histiocytic cells in the polyp stroma (IHC for S-100, ×200) (d) CD68 positivity in histiocytic cells (IHC for CD68, ×200).
The patient was scanned with Positron Emission Computed Tomography (PET-CT), which was negative for disease elsewhere in the body. Since systemic involvement was not observed, the ileal polyp was considered as a local disease and polypectomy treatment was deemed sufficient. GIT involvement is common in multisystemic disease and only a few isolated cases of GIT involvement have been reported, usually discovered incidentally in asymptomatic patients during colonoscopy performed for another reason.3
The clinical course and prognosis of the disease vary from case to case. Excision of lesions has been successful when only one organ is involved. It is recommended to administer chemotherapy in patients with multi-organ involvement.4 Generally, the prognosis is poor in patients with multifocal and multisystem disease.4 Long-term follow-up is required to exclude disease progression and systemic involvement. In adults, the prognosis is good in localised LCH.
A multi-disciplinary approach is important in treatment.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
MK, AT: Conception and design of the case; critical review of the manuscript
MK: Interpretation, and clinical diagnosis of the case and manuscript writing.
DY: Histopathological diagnosis.
All the authors have approved the final version of the manuscript to be published.
REFERENCES
- Kobayashi M, Tojo A. Langerhans cell histiocytosis in adults: Advances in pathophysiology and treatment. Cancer Sci 2018; 109(12):3707-3713. doi: 10.1111/cas.13817.
- Matsubara Y, Kobayashi M, Hijikata Y, Ota Y, Hirata Y, Ahyoung Lim L, et al. Gastrointestinal lesion in adult-onset Langerhans cell histiocytosis. Int J Clin Oncol 2020; 25(11):1945-50. doi: 10.1007/s10147-020-01739-1.
- Singhi AD, Montgomery EA. Gastrointestinal tract langerhans cell histiocytosis: A clinicopathologic study of 12 patients. Am J Surg Pathol 2011; 35(2):305-10. doi: 10.1097/PAS.0b013e31820654e4.
- Duan MH, Han X, Li J, Zhang W, Zhu TN, Han B, et al. Comparison of vindesine and prednisone and cyclophosphamide, etoposide, vindesine, and prednisone as first-line treatment for adult Langerhans cell histiocytosis: A single-center retrospective study. Leuk Res 2016; 42:43-6. doi: 10.1016/j.leukres.2016.01.012.