Effectiveness of Evidence Based Physical Therapy Management Approaches in Sacroiliac Joint Dysfunction: A Meta-analysis
By Sabrina Sabrina1, Sumaira Farooqui1, Muhammad Abid Khan1, Amna Aamir Khan1, Faisal Ali Khan2Affiliations
doi: 10.29271/jcpsp.2023.05.572ABSTRACT
Worldwide the prevalence of sacroiliac joint dysfunction (SIJD) lies within a range of 13% to 30%. In approximately 10% to 25% of patients, SIJD is a cause of mechanical low back and leg pain. A total of 498 subjects included in 10 studies conducted from 2018 to 2022 were included in this analysis. The guidelines of PRISMA were followed for study identifications and analysis in which pain and disability were monitored as an outcome measure. The results revealed statistically significant findings of physical therapy-based management approaches in decreasing pain (SMD -1.068, p=0.0001, I2=95.11%) and lowering the levels of disability (SMD -0.997, p=0.0001, I2=95.76%) among patients with SIJD as estimated using a random effect model. It was concluded that physical therapy-based management approaches ranging from combined exercise therapy to MET and K-taping are significantly more effective than traditional approaches.
Key Words: Exercise, Sacroiliac joint, Pain, Disability, Physical therapy, Muscle energy technique, Kinesiotaping.
INTRODUCTION
Worldwide, the prevalence of sacroiliac joint dysfunction (SIJD) lies within a range of 13% to 30%.1 In approximately 10% to 25% of patients, SIJD is a cause of mechanical low back and leg pain.2 Pregnancy-related low back and hip pain have been reported in 20% of women, who have chronic disabling pain in approximately 5% of cases after childbirth.3 The pathophysiology of SIJD among females has mainly dependent upon the biomechanics and angle of the joint.4 Due to less curved, posterior tilt and wider sacrum, sciatic notch, and acetabula; the risk of SIJ alignment has greatly increased among females.5 Besides that, during pregnancy the increase in axial load due to increase in abdominal and intrauterine pressure coupled with the laxity of spinal ligaments and pelvic structure greatly altered the biomechanics. Thereby, increases the risk of developing moderate to severe pain by three-fold due to SIJ dysfunction.6
SIJD pain commonly referred to back and buttocks that radiates to the knee joint.7 The aggravating factors involved standing up from sitting position and lying down, besides that the pain also exacerbates during climbing up and descending from stairs.8
Patients report stabbing pain deep into the buttocks that is often localised at the posterior side of the pelvis.8
Multiple management approaches ranging from pharmaceutical management to physiotherapy and even surgeries are recommended in extreme cases depending upon patient condition;9 but in recent decades, the prime consideration has been given to physical therapy-based management approaches for SIJD. Several physical therapy interventional approaches provided to patients for managing pain and reducing disability are often the same as those used during mechanical low back pain management. These techniques include manual therapy, cupping, muscle energy technique, K-taping, SIJ stabilisation using the sacroiliac joint belt, and electrotherapy applications that may include but are not limited to transcutaneous nerve impulse and therapeutic ultrasound.10 All of them are considered as a paramount physical therapy technique for the management of pain and disability.
Hence, based on available evidence, the present study aims to identify the impact of physical therapy-based management approaches that have recently been modified from conventional to contemporary in managing pain and disability among patients with SIJD.
METHODOLOGY
A total number of 10 studies including 498 participants were analysed following the guidelines of preferred reporting items for systematic reviews and meta-analysis (PRISMA).
Table I: Represents characteristics and features of the included studies.
|
Author’ Year |
Sample Size |
Target Population |
Study Design |
Age |
Intervention |
Outcome |
|
|
Intervention Group |
Control Group |
||||||
|
Sabrina et al., 202212 |
EG=26 CG=26 |
Postpartum women with SIJD |
RCT |
20-35 years |
Kinesio Taping |
Muscle Energy Techniques |
Pain and disability |
|
Aghalar et al., 202113 |
EG=23 CG=23 |
Women with SIJD |
RCT |
18-60 years |
Manual therapy and SIJ exercise program being performed at home |
SIJ home and lumbar exercises program, home therapy |
Pain and disability |
|
Hui et al., 202114 |
EG=48 CG=48 |
Patients with lumbopelvic pain after childbirth. |
RCT |
20 and 35 years |
Pelvic floor exercises along with TENS |
TENS only |
Pain and disability |
|
Ordahan B & Eriç Horasanlı J, 202115 |
EG=25 CG=25 |
Women with SIJD |
RCT |
X=25.60 in experimental group and X= 24.71 in Control Group |
KinesioTaping |
Sham Kinesiotaping |
Pain and disability |
|
Kamali et al., 201916 |
EG=15 CG=15 |
Patients with sub-acute or chronic SIJD |
RCT |
20 to 60 years |
Manipulation |
Conventional Physical Therapy |
Pain and disability |
|
Khobragade S et al., 201917 |
EG=37 CG=37 |
Postpartum female with SIJ pain |
RCT |
20 to 45 years |
K-taping |
Conventional training |
Pain and disability |
|
ElDeeb AM et al., 201918 |
EG=20 CG=20 |
Postpartum women with pelvic pain due to SIJ dysfunction |
RCT |
25–35 years |
Pelvis stabilisation exercises |
Conventional training |
Pain and disability |
|
Vaseghnia et al., 201919 |
EG=25 CG=25 |
Women with SIJD pain |
RCT |
18 to 40 years |
Muscle Energy Technique (MET) |
Sham positioning training |
Pain and disability |
|
Teymuri et al., 201820 |
EG=18 CG=18 |
Postpartum lumbo-pelvic pain due to SIJ dysfunction |
Single blind RCT |
X=33.55 in the experimental group and X= 36.77 in the control group |
Electrotherapy and mobilization with stabilization exercises |
Electrotherapy modalities |
Pain and disability |
|
Brizzolara et al., 201821 |
EG=12 CG=12 |
Women with SIJ Pain |
RCT |
18 to 65 years |
Lumbar Stabilisation Exercises and Lumbar Compression Belt |
Supervised Lumbar Stabilization Exercises |
Pain and disability |
|
EG denotes the Experimental group, CG denotes the Control Group. |
|||||||
Multiple searches are performed on physical therapy-based management approaches among female patients with SIJD were identified using search engines such as, Google Scholar, PEDro, MEDLINE, Cochrane Library, EMBASE, and Web of Science by using MeSH terms like physical therapy, sacroiliac joint dysfunction, pain, disability, exercise, and low back pain.
Inclusion criteria comprised of all those studies in which the effects of physical therapy-based management approaches were determined on pain intensity and levels of disability among SIJD patients and were published from 2018 to 2022 to provide the quantitative as well as qualitative analysis of the findings of most recently conducted studies. Trials in which participants underwent different surgical approaches were excluded along with all those trials that were performed on patients with SIJD but the interventional strategies other than physical therapy management were excluded from the analysis. Furthermore, unavailable full text articles and all those studies in which languages other than English were used, and all those studies for which open access had not been provided after being contacted by authors through emails were excluded. Thereafter, going through all the screening criteria (n=10) studies were analysed that had met the inclusion criteria as shown in Table I.
Assessment of the risk of biasness of included studies was performed based on Cochrane tool parameters.11 In addition, the assessment was performed for risk of allocation (randomisation and concealing), blinding (participation and outcome) data assessment (incomplete and selective reporting), and biasness of other types based on the author’s judgment.
MedCalc, statistical software version 20.112 was used for quantitative analysis. Continuous measure analysis was performed to determine the pooled effect based on standardised mean difference (SMD) at 95% of CI. The effect size was estimated using a Cohen’s rule of thumb that had categorised an effect size on three parameters; a small effect size if the values of SMD lie within the range of 0.2 to 0.5; moderate if the values found within the range of 0.5 to 0.8, and large if the values found to be greater than 0.8. For the level of heterogeneity value of I2 were used to interpret based on the random and fixed effect model (I2 <50 fixed effect, I2 >50 Random effect).
RESULTS
A sample size of 498 participants; included in 10 studies were analysed in which the effects of physical therapy-based management approaches for SIJD were estimated on disability, and pain. After searching potentially relevant published articles from six electronic databases, initially n=120 original articles were included. Further evaluation of the initially selected articles led to the exclusion of duplicated and those articles in which physical therapy management approaches estimated after joint fusion surgeries and in which other management protocols like chiropractic and massage technique were involved, hence n=30 article remains.
Table II: Shows SMD for pain on a random effect model within 95% of CI and statistical heterogeneity.
|
Study |
N1 |
N2 |
Total |
SMD |
SE |
95% CI |
t |
P |
Weight (%) |
|
|
Fixed |
Random |
|||||||||
|
Sabrina et al., 2022 |
26 |
26 |
52 |
-0.516 |
0.278 |
-1.074 to 0.0421 |
|
|
13.56 |
10.21 |
|
Aghalar Javadov et al., 2021 |
23 |
23 |
46 |
-2.335 |
0.378 |
-3.098 to -1.572 |
|
|
7.30 |
9.90 |
|
Hui et al., 2021 |
48 |
48 |
96 |
-1.392 |
0.226 |
-1.841 to -0.943 |
|
|
20.48 |
10.33 |
|
Ordahan et al., 2021 |
25 |
25 |
50 |
-2.668 |
0.386 |
-3.443 to -1.892 |
|
|
7.04 |
9.88 |
|
Kamali et al., 2019 |
15 |
15 |
30 |
0.880 |
0.373 |
0.116 to 1.644 |
|
|
7.52 |
9.92 |
|
Khobragade et al., 2019 |
37 |
37 |
74 |
1.444 |
0.259 |
0.928 to 1.960 |
|
|
15.62 |
10.25 |
|
ElDeeb et al., 2019 |
20 |
20 |
40 |
-2.496 |
0.417 |
-3.341 to -1.652 |
|
|
6.02 |
9.77 |
|
Vaseghnia et al., 2019 |
25 |
25 |
50 |
-2.137 |
0.351 |
-2.843 to -1.431 |
|
|
8.50 |
9.99 |
|
Teymuri et al., 2018 |
18 |
18 |
36 |
-1.663 |
0.380 |
-2.435 to -0.890 |
|
|
7.24 |
9.90 |
|
Brizzolara et al., 2018 |
12 |
12 |
24 |
0.0974 |
0.394 |
-0.721 to 0.915 |
|
|
6.73 |
9.85 |
|
Total (fixed effects) |
249 |
249 |
498 |
-0.867 |
0.102 |
-1.068 to -0.666 |
-8.478 |
<0.001 |
100.00 |
100.00 |
|
Total (random effects) |
249 |
249 |
498 |
-1.068 |
0.470 |
-1.991 to -0.145 |
-2.273 |
0.023 |
100.00 |
100.00 |
|
Q |
184.1767 |
|||||||||
|
DF |
9 |
|||||||||
|
Significance level |
p <0.0001 |
|||||||||
|
I2 (inconsistency) |
95.11% |
|||||||||
|
95% CI for I2 |
92.76 to 96.70 |
|||||||||
Table III: Shows SMD for disability on a random effect model within 95% of CI and Statistical Heterogeneity.
|
Study |
N1 |
N2 |
Total |
SMD |
SE |
95% CI |
t |
P |
Weight (%) |
|
|
Fixed |
Random |
|||||||||
|
Sabrina et al., 2022 |
26 |
26 |
52 |
-0.526 |
0.278 |
-1.084 to 0.0324 |
|
|
13.89 |
10.19 |
|
Aghalar Javadov et al., 2021 |
23 |
23 |
46 |
-1.665 |
0.338 |
-2.346 to -0.984 |
|
|
9.40 |
10.05 |
|
Hui et al., 2021 |
48 |
48 |
96 |
-1.131 |
0.218 |
-1.564 to -0.697 |
|
|
22.52 |
10.31 |
|
Ordahan et al., 2021 |
25 |
25 |
50 |
-3.241 |
0.427 |
-4.100 to -2.382 |
|
|
5.88 |
9.79 |
|
Kamali et al., 2019 |
15 |
15 |
30 |
0.442 |
0.360 |
-0.295 to 1.179 |
|
|
8.29 |
9.99 |
|
Khobragade et al 2019 |
37 |
37 |
74 |
2.747 |
0.322 |
2.104 to 3.389 |
|
|
10.33 |
10.09 |
|
ElDeeb et al., 2019 |
20 |
20 |
40 |
-3.213 |
0.474 |
-4.173 to -2.253 |
|
|
4.77 |
9.64 |
|
Vaseghnia et al., 2019 |
25 |
25 |
50 |
-1.701 |
0.326 |
-2.357 to -1.045 |
|
|
10.08 |
10.08 |
|
Teymuri et al., 2018 |
18 |
18 |
36 |
-1.369 |
0.364 |
-2.109 to -0.630 |
|
|
8.11 |
9.98 |
|
Brizzolara et al., 2018 |
12 |
12 |
24 |
-0.456 |
0.400 |
-1.285 to 0.373 |
|
|
6.72 |
9.88 |
|
Total (fixed effects) |
249 |
249 |
498 |
-0.821 |
0.104 |
-1.025 to -0.617 |
-7.925 |
<0.001 |
100.00 |
100.00 |
|
Total (random effects) |
249 |
249 |
498 |
-0.997 |
0.511 |
-2.001 to 0.00791 |
-1.949 |
0.052 |
100.00 |
100.00 |
|
Q |
212.0917 |
|||||||||
|
DF |
9 |
|||||||||
|
Significance level |
p <0.0001 |
|||||||||
|
I2 (inconsistency) |
95.76% |
|||||||||
|
95% CI for I2 |
93.82 to 97.09 |
|||||||||
After further analysis, all those articles that were published before 2018, not available in English language, did not have their full-text available even after contacting the authors, and all paid articles were excluded. Finally, ten studies were included for analysis. Flow of studies is illustrated in Figure 1.
The findings from ten randomised controlled trials revealed that the physical therapy intervention showed significant improvement in decreasing pain in comparison to the control group. Standardised mean difference suggested an effect size of -1.068 in random effect model (I2 = 95.11%; p <0.0001) depicted a large effect size suggesting the beneficial effects of physical therapy in the management of pain among SIJD patients (Table II).
The diagrammatic illustration of the effect size of individual studies and the pooled effect at fixed and random effect model of studies was demonstrated in forest plot Figure 2.
A total of ten studies were analysed through continuous measure analysis, SMD to determine the effect size. The analysis revealed a random effect size of -0.997 (I2 = 95 .76%; p <0.0001) which is a larger effect, hence favouring physical therapy as an effective tool in decreasing disability among SIJD patients (Table III).
The diagrammatic illustration of the effect size of individual studies and the pooled effect at fixed and random effect model of studies was demonstrated in forest plot Figure 3.
Author’s judgment of risk of bias analysis based on guidelines of Cochrane was provided in Figure 4. The randomisation sequence analysis suggested that all nine studies revealed low risk of bias.12-21 All studies under this parameter revealed low risk of all allocation concealment bias as per author’s judgment.12-21 Seven studies considered the participants blinding,13-16,18-20 whereas, two studies reflected unknown approach.12,17,20 Four studies showed high risk of outcome assessment blinding bias,12,13,16,21 six studies14,15,17-19 showed low risk of bias, and only one study represented unknown risk.17 Four studies showed high risk of bias,12-14,16 while the remaining represented low risk for incomplete outcome data.15,17-21 All studies reflected low selection bias risk.
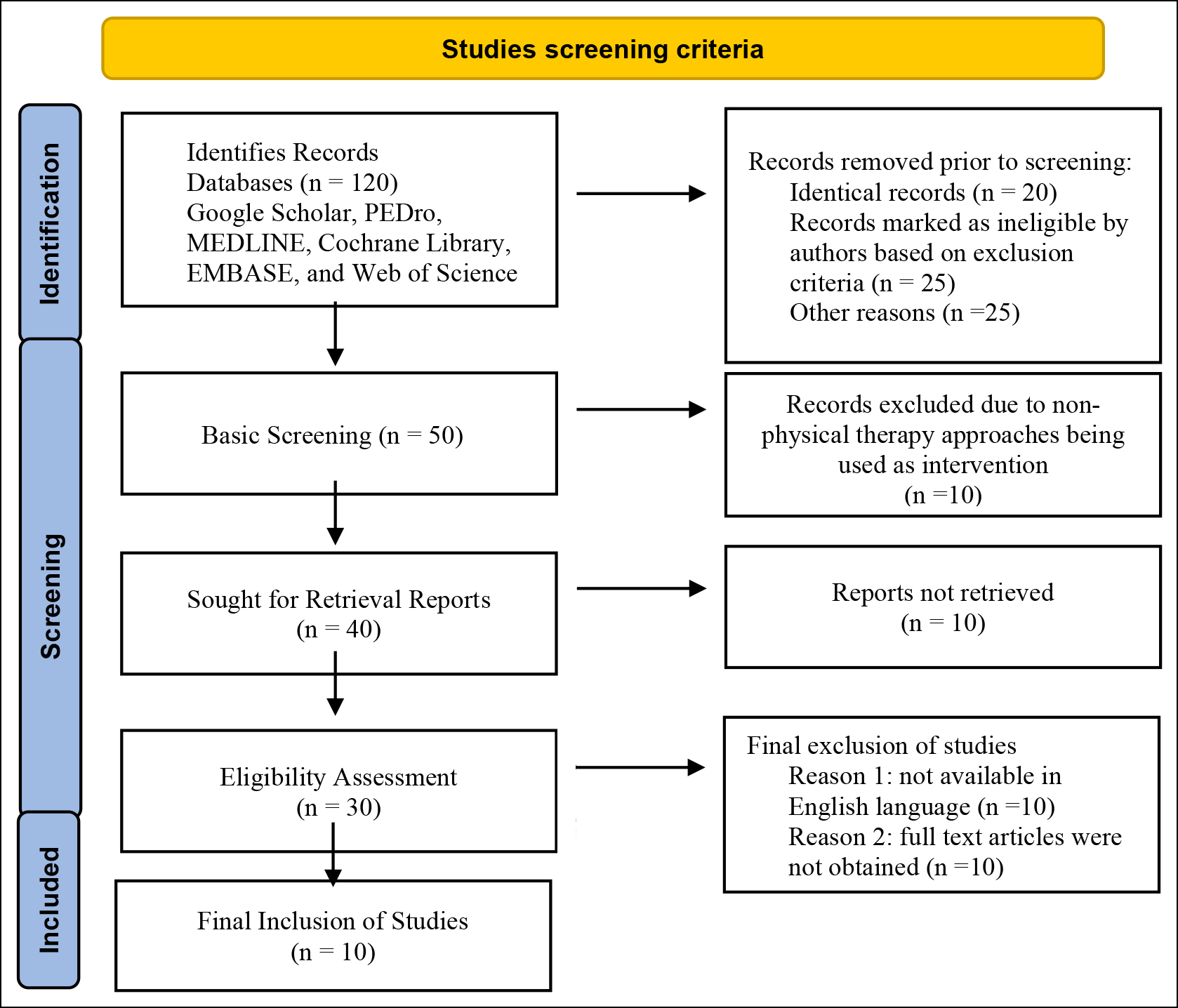 Figure 1: Represents flow of studies in accordance to PRISMA statement.
Figure 1: Represents flow of studies in accordance to PRISMA statement.
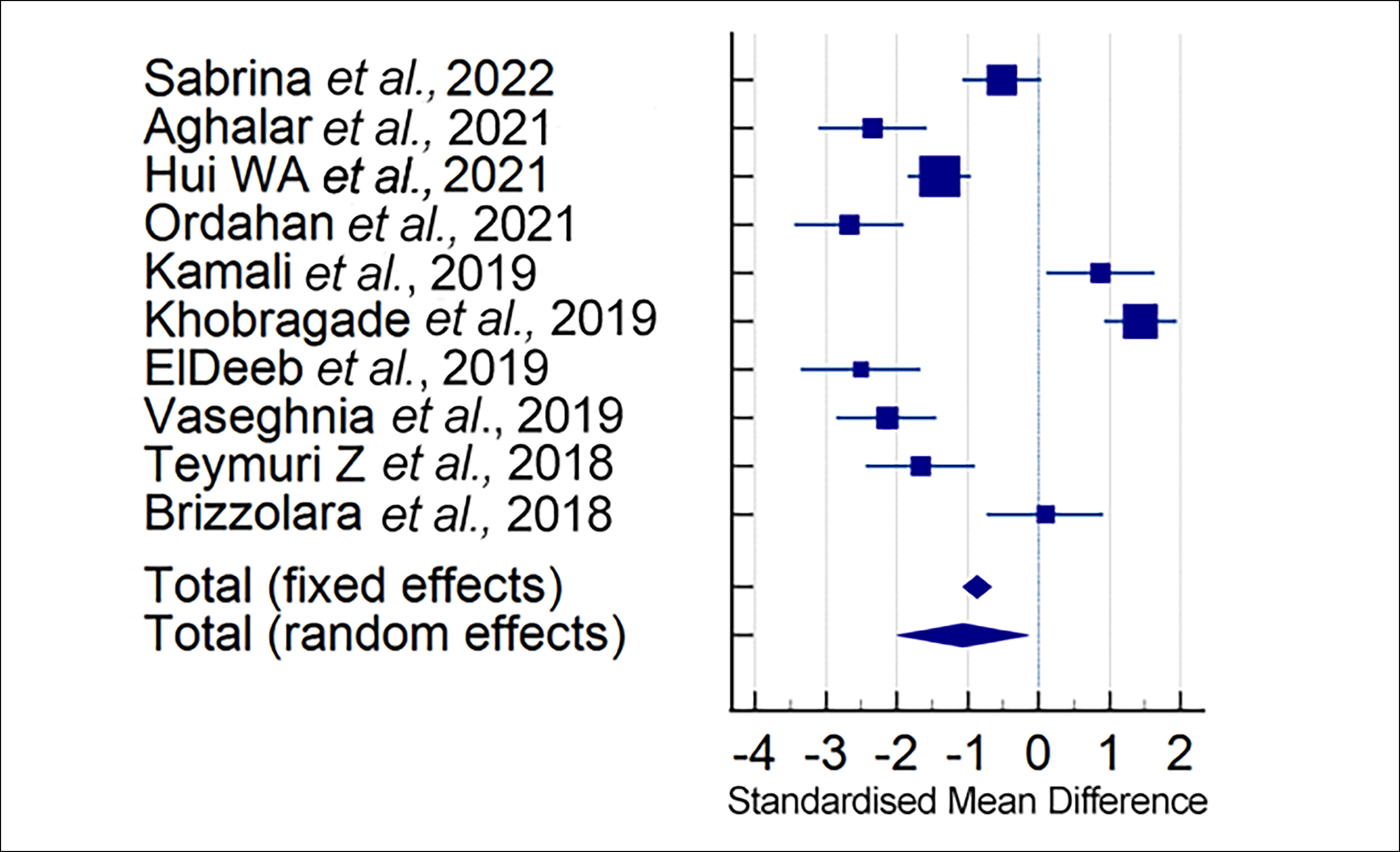 Figure 2: Represents studies that reported significantly decrease in pain among patients of SIJ dysfunction.
Figure 2: Represents studies that reported significantly decrease in pain among patients of SIJ dysfunction.
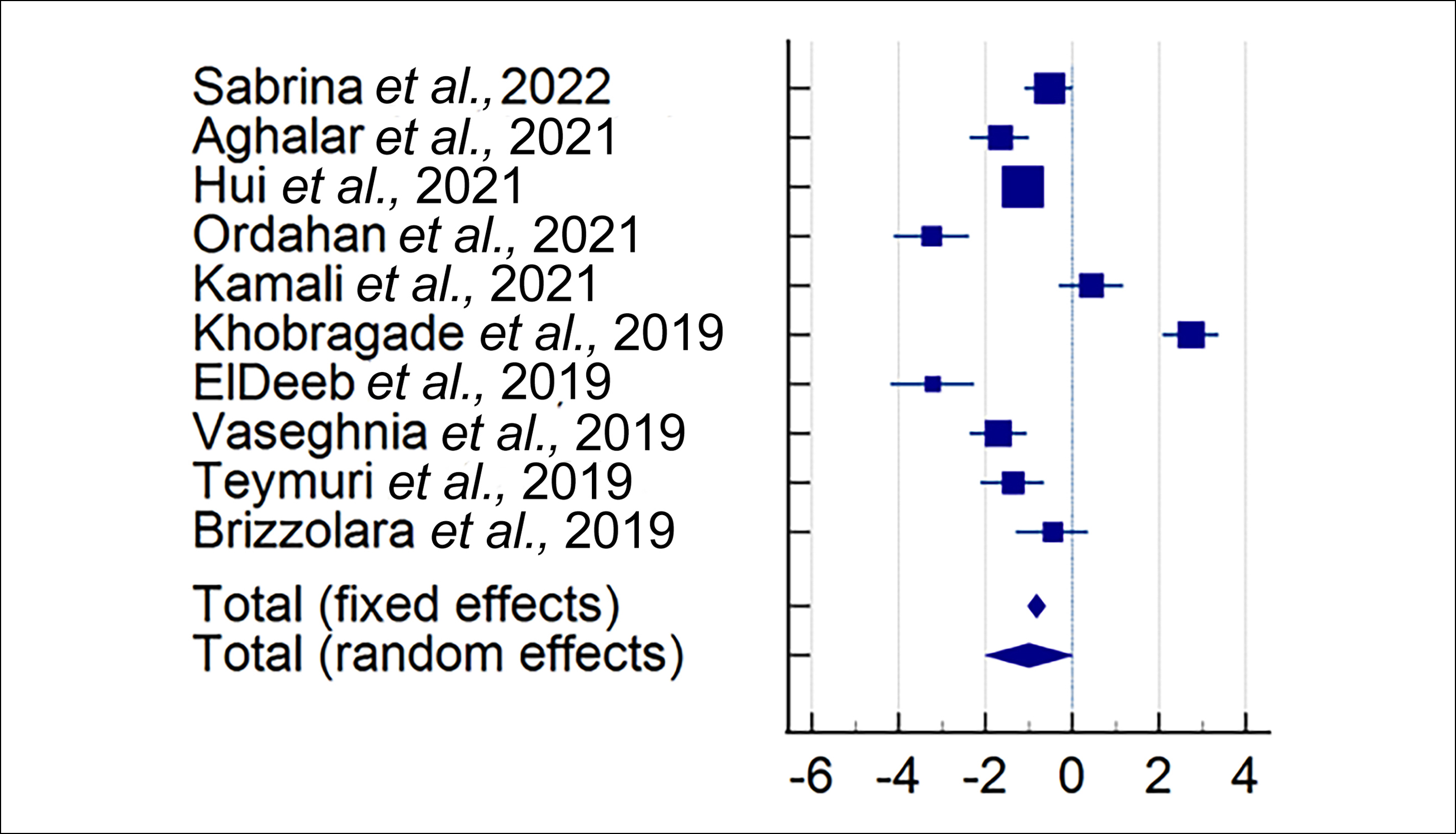 Figure 3: Represents studies that reported significantly decrease disability among patients of SIJD.
Figure 3: Represents studies that reported significantly decrease disability among patients of SIJD.
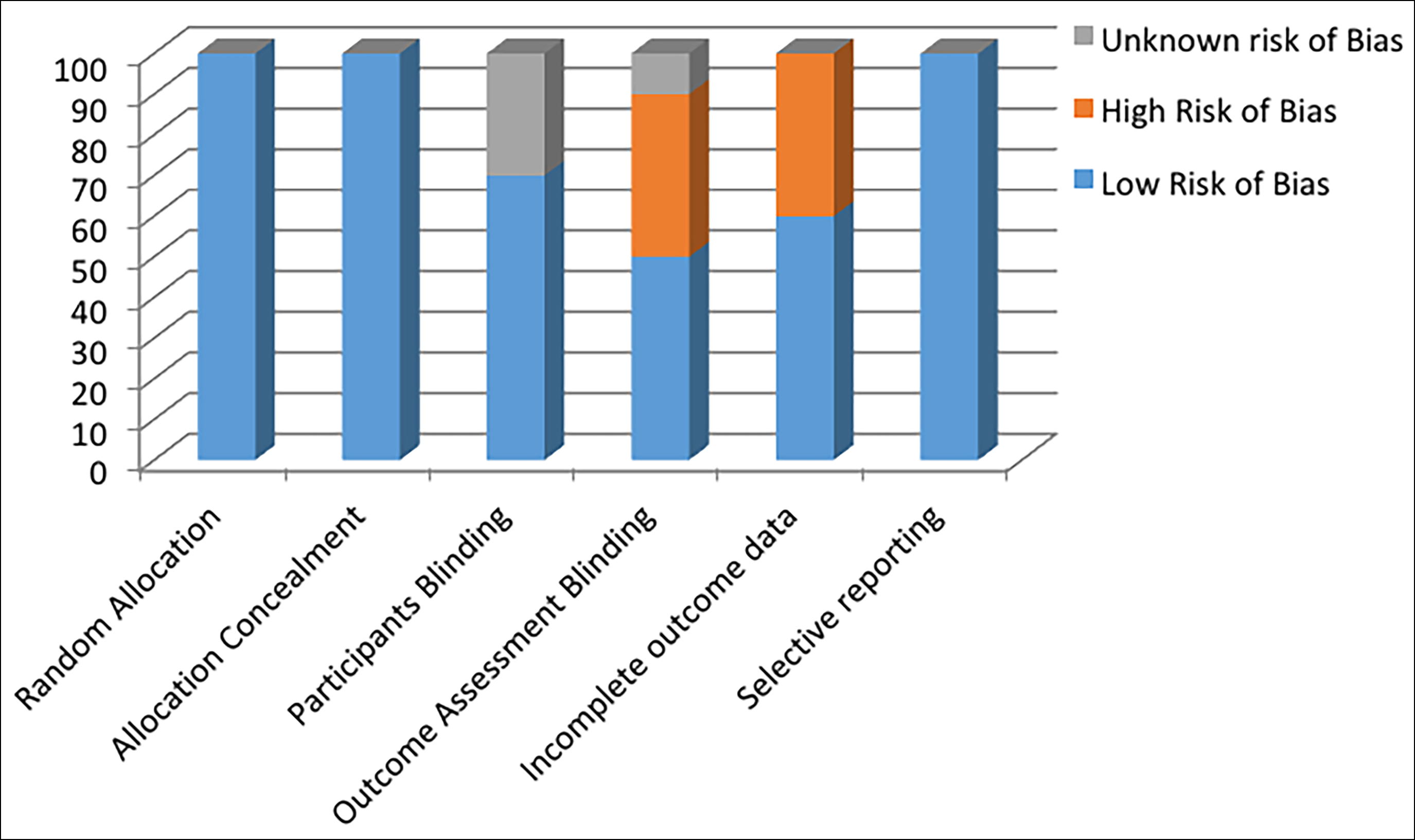 Figure 4: Represents risk of bias.
Figure 4: Represents risk of bias.
DISCUSSION
The analysis of the studies included in this review article has provided evidence that physical therapy-based management approaches incorporating newly devised techniques and combination therapies that have provided effective results as evaluated through the random effect model. The result of this review article has revealed an effect size of 0.470 (CI -1.991 to -0.145) suggesting a significant decrease in pain among all the subjects included in the literature review. Besides that, the impact of various physical therapy-based management approaches on decreasing the level of disability has also been reflected and has revealed an effect size of 0.511 (CI -2.001 to 0.00791) signifying a positive effect of physical therapy-based management approaches on disability as well. The findings of this study were according to the findings of some other reviews as well in which it has been observed that physical therapy-based management approaches were found to be effective in managing pain and disability.22 Besides, considering various randomised controlled trials in which two different physical therapy-based approaches have been used in managing pain and disability, the authors have reported significant findings, particularly in low back pain.23,24 Similarly, studies included in this meta-analysis elaborated the effects of modified evidence-based exercises regimes in managing pain and disability among SIJD patients. Combination of therapies such as electrotherapy and mobilisation,21 manual therapy along with home program,13 pelvic floor exercises in combination with TENS, were all turned out to be more effective than individual therapies alone and the convention physical therapy approaches. Likewise, application of kinesiotape (KT) alone was found to be more effective than sham KT and conventional exercises.15,17 Moreover, pelvic stabilisation exercises and MET exercises had also shown better results in reducing pain and lowering disability among SIJD patients.12,19 In a systematic review conducted to determine the effects of non-surgical management approaches for excessive pelvic tilt, the authors had observed no conclusive evidence thus, revealing that high-quality interventional studies are required for better findings.25 On the contrary, this meta-analysis observed strong evidence of physical therapy-based management approaches in relieving pain and lowering the level of disability. Hence, it was suggested that physical therapy management must be incorporated as an independent or adjunct management approach for SIJD.
CONCLUSION
Physical therapy-based management approaches ranging from combining exercise therapy to MET and K-taping were found to be significantly effective than traditional approaches of combining electrotherapy and exercise approaches in managing pain and disability. Evidence-based physical therapy protocols are more effective than conventional physical therapy approaches. Therefore, these can be used as alternative and adjunct approaches to managing pain and disability among patients with SIJD.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
SS: Conception and design of work.
SF, MAK: Analysis of data, drafting of work, and critical review.
AAK: Final approval of the manuscript.
FAK: Revision of the manuscript and questions related to integrity.
All the authors have approved the final version of the manuscript to be published.
REFERENCES
- Srivastava S, KU DK, Mittal H, Dixit S, Nair A. Short-term effect of muscle energy technique and mechanical diagnosis and therapy in sacroiliac joint dysfunction: A pilot randomised clinical trial. J Bodyw Move Ther 2020; 24(3):63-70. doi: 10.1016/j.jbmt.2020.02.017.
- Thawrani DP, Agabegi SS, Asghar F. Diagnosing sacroiliac joint pain. J Am Aca Orthop Surg 2019; 27(3):85-93. doi: 10.5435/JAAOS-D-17-00132.
- Kiil RM, Arnbak BA, Zejden A, Schiøttz-Christensen B, Hendricks O, Jurik AG. Pregnancy-related sacroiliac joint findings in females with low back pain: A four-year magnetic resonance imaging follow-up study. Acta Radiol 2022; 63(6):775-84. doi: 10.1177/02841851211017108.
- Kiapour A, Joukar A, Elgafy H, Erbulut DU, Agarwal AK, Goel VK. Biomechanics of the sacroiliac joint: Anatomy, function, biomechanics, sexual dimorphism, and causes of pain. Int J Spine Surg 2020; 14(Suppl 1):S3-13. doi: 10.14444/6077.
- Joukar A, Shah A, Kiapour A, Vosoughi AS, Duhon B, Agarwal AK, et al. Gender specific sacroiliac joint biomechanics during standing upright: A finite element study. Spine (Phla Pa 1976) 2018; 43(18):E1053-60. doi: 10.1097/BRS.00000 00000002623.
- Fiani B, Sekhon M, Doan T, Bowers B, Covarrubias C, Barthelmass M, et al. Sacroiliac joint and pelvic dysfunction due to symphysiolysis in postpartum Women. Cureus 2021; 13(10):18619. doi: 10.7759/cureus.18619.
- Schneider BJ, Rosati R, Zheng P, McCormick ZL. Challenges in diagnosing sacroiliac joint pain: A narrative review. PMR 2019; 11:S40-5. doi: 10.1002/pmrj.12175.
- Falowski S, Sayed D, Pope J, Patterson D, Fishman M, Gupta M, Mehta P. A review and algorithm in the diagnosis and treatment of sacroiliac joint pain. J Pain Res 2020; 13:3337. doi: 10.2147/JPR.S279390.
- Zaidi F, Ahmed I. Effectiveness of muscle energy technique as compared to Maitland mobilization for the treatment of chronic sacroiliac joint dysfunction. J Pak Med Assoc 2020; 70(10):37-8.
- Anbar AR, Saleh AM, Ismail NM, El-Shazly U. Cupping versus kinesiotap on management of patients with sacroiliac joint dysfunction: A randomised controlled trial. Delta University Scientific J 2020; 3(2):21-32.
- Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011; 343:d5928. doi: 10.1136/bmj.d5928.
- Sabrina, Farooqui SI, Khan MA, Khan AA, Hameed A, Khan FA. The effectiveness of kinesio-taping and muscle energy technique among postpartum females with Sacro-iliac joint dysfunction. Med Forum 2022; 33(10):96-9.
- Javadov A, Ketenci A, Aksoy C. The efficiency of manual therapy and sacroiliac and lumbar exercises in patients with sacroiliac joint dysfunction syndrome. Pain Physician 2021; 24(3):223-3.
- Hui WA, Xiaolan FE, Zishu LI, Yan LI. A rehabilitation programme focussing on pelvic floor muscle training for persistent lumbopelvic pain after childbirth: A randomised controlled trial. J Rehabil Med 2021; 53(4). doi: 10.2340/ 16501977-2812.
- Ordahan B, Eriç Horasanlı J. Effectiveness of kinesiotaping in pregnant women with sacroiliac joint pain: A randomised controlled study. Int J Clin Prac 2021; 75(9):e14432. doi: 10.1111/ijcp.14432.
- Kamali F, Zamanlou M, Ghanbari A, Alipour A, Bervis S. Comparison of manipulation and stabilisation exercises in patients with sacroiliac joint dysfunction patients: A randomised clinical trial. J Bodyw Mov Ther 2019; 23(1): 177-82. doi: 10.1016/j.jbmt.2018.01.014.
- Khobragade S, Naqvi W, Dhankar S, Jungade S. Impact of K-Taping on sacroiliac joint pain in women after full-term normal delivery. J Datta Meghe Institute Med Sci Uni 2019; 14(4):352.
- ElDeeb AM, Abd-Ghafar KS, Ayad WA, Sabbour AA. Effect of segmental stabilizing exercises augmented by pelvic floor muscles training on women with postpartum pelvic girdle pain: A randomised controlled trial. J Back Musculoskeletal Rehabil 2019; 32(5):693-700.
- Vaseghnia A, Shadmehr A, Moghadam BA, Olyaei G, Hadian MR, Khazaeipour Z. Effects of muscle energy technique on daily activities and lumbar stiffness in women with sacroiliac joint dysfunction: A randomised controlled clinical trial study. J Modern Rehabil 2019; 13(1):23-30.
- Teymuri Z, Hosseinifar M, Sirousi M. The effect of stabilization exercises on pain, disability, and pelvic floor muscle function in postpartum lumbopelvic pain: A randomised controlled trial. Am J Phys Med Rehabi 2018; 97(12):885-91. doi: 10.1097/PHM.0000000000000993.
- Brizzolara KJ, Wang-Price S, Roddey TS, Medley A. Effectiveness of adding a pelvic compression belt to lumbopelvic stabilization exercises for women with sacroiliac joint pain: A feasibility randomised clinical trial. J Women’s Health Phys Ther 2018; 42(2):76-86.
- Wallace SL, Miller LD, Mishra K. Pelvic floor physical therapy in the treatment of pelvic floor dysfunction in women. Curr Opin Obstet Gynecol 2019; 31(6):485-93. doi: 10.1097/ GCO.0000000000000584.
- Seo UH, Kim JH, Lee BH. Effects of mulligan mobilization and low-level laser therapy on physical disability, pain, and range of motion in patients with chronic low back pain: A pilot randomised controlled trial. Healthcare (Basel) 2020; 8(3):237. doi: 10.3390/healthcare8030237.
- Areeudomwong P, Buttagat V. Proprioceptive neuro-muscular facilitation training improves pain-related and balance outcomes in working-age patients with chronic low back pain: A randomised controlled trial. Braz J Phys Ther 2019; 23(5):428-36. doi: 10.1016/j.bjpt.2018.10.005.
- Brekke AF, Overgaard S, Hróbjartsson A, Holsgaard-Larsen A. Non-surgical interventions for excessive anterior pelvic tilt in symptomatic and non-symptomatic adults: A systematic review. EFORT Open Rev 2020; 5(1):37-45. doi: 10.1302/2058-5241.5.190017.