Cecal Diverticulitis: A Diagnosis to Keep in Mind When Evaluating Acute Appendicitis
By Hakan BolukbasiAffiliations
doi: 10.29271/jcpsp.2022.08.1067ABSTRACT
Cecal diverticulitis is a rare cause of right lower-quadrant abdominal pain. As its symptoms mimic those of acute appendicitis, the final diagnosis in the patients is generally confirmed after surgery. Herein, we report a 45-year man who was admitted to the department of emergency with lower right abdominal pain. Cecal diverticulitis was diagnosed on computed tomography (CT) images, and a conservative treatment approach was recommended. He was hospitalised, and intravenous antibiotics and hydration were administered immediately. Oral feeding was interrupted. After five days of intensive medical care, the patient was discharged without any further complications. Based on my experience, I advise that CT can be used to differentiate cecal diverticulitis from the acute appendicitis. In uncomplicated cases, conservative approaches are advised.
Key Words: Cecal diverticulitis, Computed tomography, Acute appendicitis, Conservative treatment.
INTRODUCTION
Cecal diverticulitis a rare diagnostic entity, accounting for about 3.6% of all the colonic diverticulosis cases with a incidence in the median age of 44 years and a male-to-female ratio of 3:2.1 The most important complication is diverticulitis which usually presents in a manner similar to that of acute appendicitis. It is hardly differentiated on imaging such as abdominal ultrasound (US) and computed tomography (CT), but surgery reveals the diagnosis of cecal diverticulitis.2,3 Both US and CT have been shown to confer high diagnostic accuracy and may play a role in preoperative diagnosis. CT scans are very common and accessible. Therefore, the preoperative accuracy rate of CT scan in distinguishing acute appendicitis from cecal diverticulitis has been reported to have a sensitivity and specificity of 98%.1,3
We, herein, report a case of cecal diverticulitis that was correctly detected on preoperative CT and discuss the literature in the light of diagnostic and treatment options.
CASE REPORT
A 45-year man was admitted to the emergency department with right lower abdominal pain that persisted for two days. He denied vomiting, nausea, and loss of appetite. No co-morbidities or surgeries were reported in his medical history. On evaluation, his heart rate was 80 beats/min, blood pressure, was 140/85 mmHg, and he had fever with a body temperature of 37.5°C.
Physical examination revealed tenderness in the right iliac fossa associated with guarding and local peritonitis. All the other systems were normal. Diagnostic abdominal US imaging revealed no intraperitoneal fluid, but the appendix was not visualised due to the presence of gas. Based on this result, CT scans of the abdomen were ordered, indicating solitary cecal diverticulosis and inflammation of the pericolic mesenteric fat tissue and colon (Figure 1). His laboratory findings were: White blood cell count, 13.5 × 109/L, and C-reactive protein, 220 mg/L.
Based on the diagnosis of cecal diverticulitis, he was hospitalised and decided to continue with a conservative treatment approach. Oral food intake was stopped, and intravenous fluids, antibiotics, and analgesics were administered for five days. He was discharged on the fifth day without any symptoms. Colonoscopy was performed in the 6th week of the follow-up. Figure 2 shows the colonoscopy findings. No pathology was detected. He had no disease or symptoms in the third-year after hospitalisation.
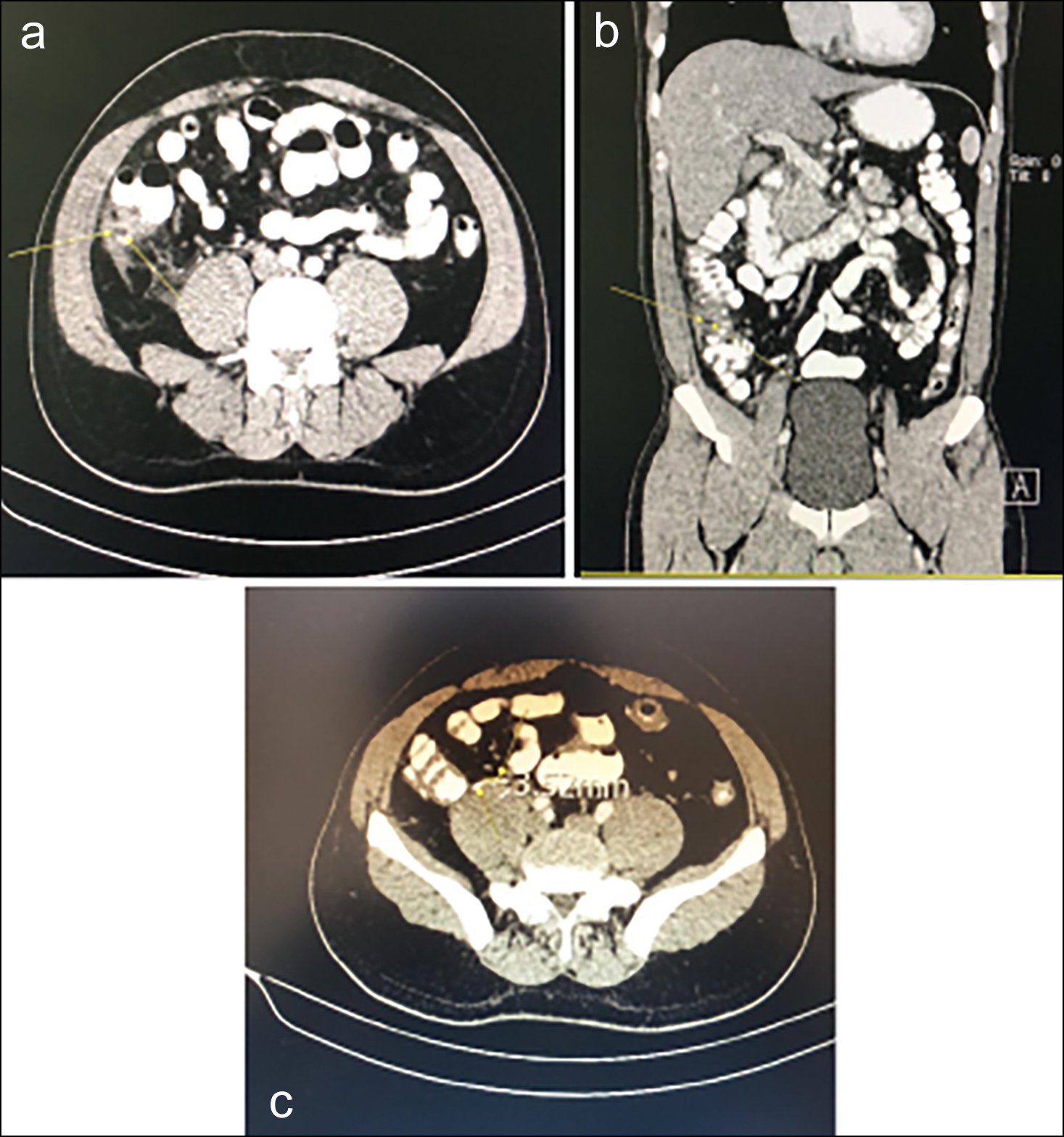 Figure 1: (a) Axial, (b) coronal CT images showing diverticulum (yellow arrow), and (c) normal appendix on CT axial image 3.2 mm in size which was reported as normal.
Figure 1: (a) Axial, (b) coronal CT images showing diverticulum (yellow arrow), and (c) normal appendix on CT axial image 3.2 mm in size which was reported as normal.
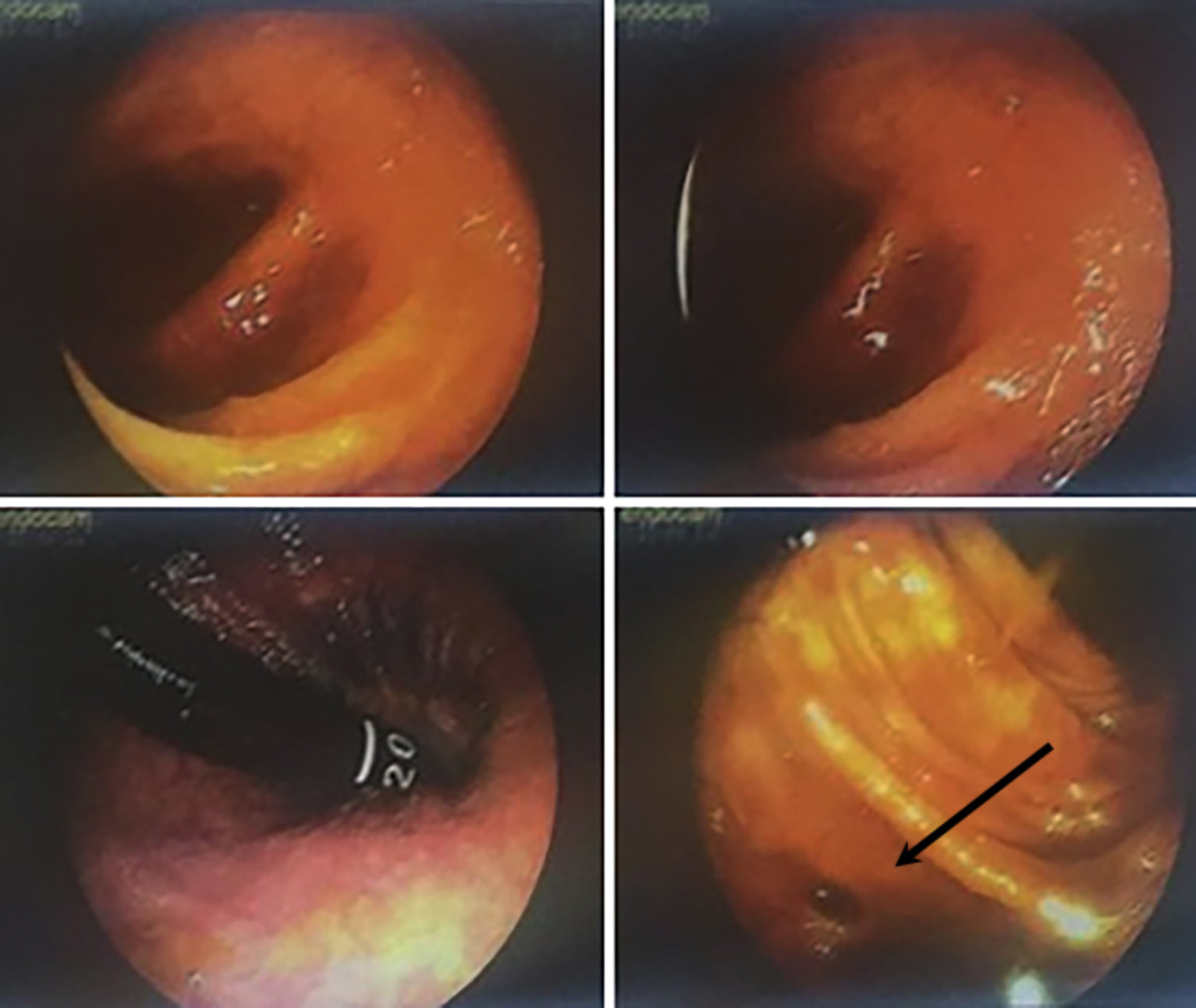 Figure 2: Endoscopic images showing cecal diverticulum. Arrow reveals the display of an endoscopic view with a round-shaped mouth of diverticulum.
Figure 2: Endoscopic images showing cecal diverticulum. Arrow reveals the display of an endoscopic view with a round-shaped mouth of diverticulum.
DISCUSSION
In clinical practice, it is generally difficult to differentiate cecal diverticulitis from the acute appendicitis based on clinical and laboratory findings. Cho et al. emphasised the importance of clinical symptoms such as nausea and vomiting which are reported less-frequently in patients with cecal and right-sided colonic diverticulitis (26.7%) compared to the frequency in patients with appendicitis (51%).4 In classical appendicitis, complaints of pain and rebound tenderness at McBurney's point are demonstrated. In contrast to this finding, Lauridsen and Ross reported that the patients with diverticulitis present with the complaints of pain and rebound tenderness that are not clearly localised.5 As leukocytosis can be detected in 58% of the patients with cecal diverticulitis and in 90% of the patients with appendicitis, leukocytosis, and elevated C-reactive protein levels may confer less specificity for determining the correct diagnosis.6 Despite these results, some case reports have revealed that moderately elevated levels of leukocytes and higher percentages of lymphocytes may be indicators of cecal diverticulitis.7 The patient denied any prodromal symptoms such as nausea and vomiting, the pain originated in the middle of the abdomen, and his leukocyte elevation was mild.
The US is a user-dependent imaging system therefore, the sensitivity and specificity may increase proportionally to the experience of the user. As cecal diverticulitis is a rare disease, prior encounters with such cases are the most important component for its diagnosis. In addition, I observed the presence of gas that blurred the optimum conditions of US imaging. Thus, obesity, abdominal tension, and gas may negatively affect accurate evaluation. Based on this, I proceeded with a CT scan. In the literature, almost 75% of the reported cecal diverticulitis cases involve a misdiagnosis of the acute appendicitis, and only 6% involved the correct diagnosis before any surgery.8
CT images have more detailed anatomical information to distinguish right colonic diverticula, specifically in the cecal region from acute appendicitis with 98% sensitivity and specificity.9 In the clinical routine, we do not perform CT scans for all the patients. If the physical examination and hematological findings do not differentiate between acute appendicitis and cecal diverticultis, a CT scan for further evaluation is suggested. Diagnosis based on the findings of the CT scan and the surgery was cancelled. Depending on this, we suggest obtaining CT images in cases of unclear US results and blood tests.
The treatment of cecal diverticulitis consists of a variety of approaches from conservative management to aggressive surgery. Conservative treatment with antibiotics may result in recurrences at the rate of 25%. If surgery is needed, diverticulectomy, ileocecal resection, or right hemicolectomy with primary anastomosis may be options depending on the operative findings.10 The patient was correctly diagnosed preoperatively on a CT scan, underwent conservative medical treatment, and was followed up without any recurrences for the three years.
PATIENT’S CONSENT:
Written informed consent was obtained from the patient and the family to report this case study.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHOR’S CONTRIBUTION:
HB: Involved in the conception, design and interpretation, wrote the manuscript, collected data, reviewed relevant published reports, and provided the images. Read and approved the final manuscript.
REFERENCES
- Sardi S, Gokli A, Singer JA. Diverticular disease of the caecum and ascending colon. A review of 881 cases. Am Surg 1987, 53:41-5. PMID: 3099619.
- Chiu PW, Lam CY, Chow TL, Kwok SP. Conservative approach is feasible in the management of acute diverticulitis of the right colon. Aust NZ J Surg 2001; 71:634-6. doi: 10.1046/j.1445-1433.2001.2226.x.
- Kurer MA. Solitary cecal diverticulitis as an unusual cause of right iliac fossa mass: Case report. J Med Case Rep 2007; 1:132-10. doi: 10.1186/1752-1947-1-132.
- Cho HJ, Cho SY, Oh JH. Clinical analysis of right colonic diverticulitis that was operated under the impression of acute appendicitis. J Korean Soc Coloproctol 2000; 16:18-24.
- Lauridsen J, Ross FP. Acute diverticulitis of the cecum; a report of four cases and review of one hundred fifty-three surgical cases. AMA Arch Surg 1952; 64:320-30. PMID: 14894054.
- Suh KW, Suh YJ, Choi JS, Yoo CH, Kim JH. Clinically differential diagnosis of cecal diverticulitis from appendicitis. J Korean Surg Soc 1996; 12:94-8.
- Shin JH, Son BH, Kim H. Clinically distinguishing between appendicitis and right-sided colonic diverticulitis at initial presentation. Yonsei Med J 2007; 48:511-16. doi: 10.3349/ ymj.2007.48.3.511.
- Lee KJ, Hyun TI. Clinical evaluation of colonic diverticular disease. J Korean Surg Soc 1995; 11:100-6.
- Cole M, Ayantunde AA, Payne J. Cecal diverticulitis presenting as acute appendicitis: A case report. World J Emerg Surg 2009; 4:298. doi: 10.1186/1749-7922-4-29.
- Papaziogas B, Makris J, Koutelidakis I, Paraskevas G, Oikonomou B, Papadopoulos E, et al. Surgical management of cecal diverticulitis: Is diverticulectomyenough? Int J ColorDis 2005; 20:24-7. doi: 10.1007/s00384-004-0630-4.