Caregiver Strain and its Associated Factors in Autism Spectrum Disorder in Karachi, Pakistan
By Rabeeka Aftab, Shahina Pirani, Marium Mansoor, Tania NadeemAffiliations
doi: 10.29271/jcpsp.2023.07.784ABSTRACT
Objective: To determine the frequency of caregiver strain and its associated factors in Autism Spectrum Disorder (ASD) at a tertiary care teaching hospital in Karachi, Pakistan.
Study Design: An analytical cross-sectional study.
Place and Duration of the Study: Psychiatry inpatient and outpatient units at The Aga Khan University Hospital, Karachi, Pakistan, from December 2018 to December 2019.
Methodology: The study participants were caregivers of ASD. Data were collected from the inpatient and outpatient departments using Caregiver Strain Questionnaire (CGSQ), and a demographic questionnare. Data were analysed using descriptive and inferential analysis.
Results: A total of 76 caregivers participated in the study. Among them, 61 (80.3%) were females and 15 (19.7%) were males, with mean age of 37.09±6.91 years. The overall caregiver strain (both subjective and objective) was reported to be severe by 11.8%, moderate by 47.4% and low by 40.8%. About 50% of the participants had a low objective strain on CGSQ whereas 59.2% of the participants subjectively felt the strain to be at moderate level. An association was found between the gender of the participants and subjective strain (p=0.016), and gender with internalised subjective strain (p =0.002).
Conclusion: Parenting of a child with ASD involves challenges and demands support. This study supports the recommendation that the caregivers need access to appropriate means to channelize their strain and manage their role productively.
Key Words: Autism, ASD, Stress, Burden, Caregiver, CGSQ, Pakistan
INTRODUCTION
Autism spectrum disorders (ASD) are pervasive, neurodevelopmental, and clinically complex disorders, characterised by deficits in social interaction and communication, accompanied by restricted, repetitive patterns of behaviour, interests, or activities.1 ASD is believed to transcend socio-cultural, racial, ethnic, and geographic boundaries. In 2022, the World Health Organization (WHO) estimated the global prevalence of ASD to be 1 in 100 children.2 In South Asia, one out of 93 children, has ASD.3 A study in semi-urban India reported ASD prevalence as 0.23%.4 In Pakistan, prevalence studies were limited to either hospitals or special schools, and therefore it is hard to generalise the results. According to the Pakistan Autism Society estimates, around 350,000 children in Pakistan have this disorder.5
ASD as a lifelong condition involves persistent impairments in several domains leading to stressors for the primary caretakers, specifically mothers. Children with ASD often need more specialised and long-term medical care in addition to primary care. Various timely interventions are required to help with clinical presentations such as impaired social communication and skills, executive functioning deficits, issues with sensory perception, motor skills, and perspective-taking, along with restricted interests and co-occurring psychiatric diagnoses.6 The time between recognition of symptoms by caregivers and diagnosis averaged about 2 years in the literature.
Out of all the people who have ASD, some can lead independent lives, while most have symptoms that interfere greatly with the quality of life, thus requiring extensive caregiving. They frequently present with a variety of emotional and behavioural problems ranging from sleep issues, toileting, eating problems, hyperactivity, sensory difficulties, anxiety, tantrums, aggression towards others, and self-injurious behaviours which can be challenging for families and healthcare providers.7
The caregivers are known to experience various challenges, often associated with their caregiving role. A study in Iraq showed a significant psychosocial burden in caregivers of ASD patients.8 A study was conducted in India to determine the prevalence of psychiatric morbidity and caregiver burden among primary caregivers of patients with psychiatric illness, showing significant results.9 A study conducted in Lahore, Pakistan, which aimed to studying factors associated with stress among parents of autistic children revealed the severity of a child's impairment as the most salient risk factor for parenting stress.10
Caregiver strain negatively affects the physical, psychological, emotional, and functional health of the caregivers.11 It reflects the caregiver’s perceived pressure associated with tasks and responsibilities and also their level of distress.12 Caregivers have previously reported social strain, disrupted family life, and negative effects on their health.13
It is important to identify the areas of strain and provide adequate support as caregivers of children with ASD may encounter a unique set of challenges that are not faced by caregivers of children without ASD. Failure to address these challenges can potentially impact the quality of life for both.14 The present study aimed to determine the associated factors of caregiver strain in Autism Spectrum Disorders at a tertiary care teaching hospital in Karachi, Pakistan.
METHODOLOGY
An analytical cross-sectional study was conducted among caregivers of ASD, recruited from the inpatient and the outpatient Psychiatry units at The Aga Khan University Hospital, Karachi, Pakistan. The inclusion criteria for the study participants were caregivers of ASD patients, irrespective of gender, within the age limit 18-65 years presented at the study setting with duration of diagnosis of ASD greater than or equal to 6 months, willing to participate, and provided written informed consent. The exclusion criteria were caregivers who were suffering from serious medical or surgical conditions, refused to participate, and did not provide consent. Before commencing the study, ethical approval was obtained from The Aga Khan University Hospital's Ethical Review Committee (reference number 2019-1673-4089). Permission to collect the data was sought from the Head of the study setting.
Taking frequency of caregiver strain as 18%15 and precision of 8% with 95% confidence interval and based on the least sample size proportion of outcome variable, the estimated sample size for this study came out to be 89 patients. An additional 10% of patients were included to cater for non-responders. Therefore, the total sample size was rounded off to 100 patients. The study duration was decided to be 12 months. Hence, 100 participants or 12-month study duration whichever was achieved first.
Using convenience sampling, the eligible participants were recruited and provided with information about the purpose, risks, benefits of the study, and their rights as participants. Those participants who were willing and interested to participate were interviewed after obtaining written informed consent. The data collection was done using a demographic questionnaire and Caregiver Strain Questionnaire (CGSQ).16 A demographic questionnaire was used to elicit participants’ information including age, gender, occupation, marital status, family structure, and so on. CGSQ is used to capture both the subjective and objective aspects of caregiver strain. It is a validated tool to measure caregiver burden amongst caregivers of children with ASD.17 The objective strain consists of eleven items that assess observable negative events. Subjective strain measures emotional responses that are divided into the subjective externalised scale and subjective internalised strain. The data collection was done at a discrete place in the Psychiatry Department for the period 12 months. The duration of each interview was 10-15 minutes.
Data were entered and analysed in the Statistical Package for Social Sciences 19.0. Mean and Standard Deviation were computed for continuous variables and frequencies were calculated for categorical variables. Post-stratification chi-square test was used to see the effect on outcome variables. A p-value of <0.05 was taken as significant.
RESULTS
A total of 76 caregivers participated in the study. Among them, 80.3% (n=61) were females and 19.7% (n=15) were males. The mean age of participants was 37.09 of ± 6.911 years. All except one of the participants were parents of the patients. Regarding education level, 46% (n=35) of participants were graduates and 39.5% (n=30) were postgraduates. Around 69.7% (n=53) of the participants were unemployed, out of which 11.4% left employment after their child was diagnosed to have ASD. Out of 30.3% employed participants, 21.1% (n=16) were professionals and 7.9% (n=6) had businesses of their own. Around 17.1% (n=13) of the participants had a diagnosed medical/ surgical or psychiatric condition. More than half of the participants lived in a nuclear family setup, while 40.8% (n=31) lived in a joint family system. Around 50% (n=38) of the cohort was taking care of the patient independently and the remaining 50% (n=38) had other family member’s help.
With regards to patients' (children with ASD) demographic information, the mean age was 7.09 years with a standard deviation of ± 4.306. Among them, 92.1% (n=70) were males and 7.9% (n=6) were females. Of them, 51.3% (n=39) of the patients were students, and 80% (n=61) were studying in pre-nursery classes. Around 71.1% (n=54) of the patients attended therapy centres for either speech therapy, occupational therapy, social skills training, behavioural therapy or a combination of them.
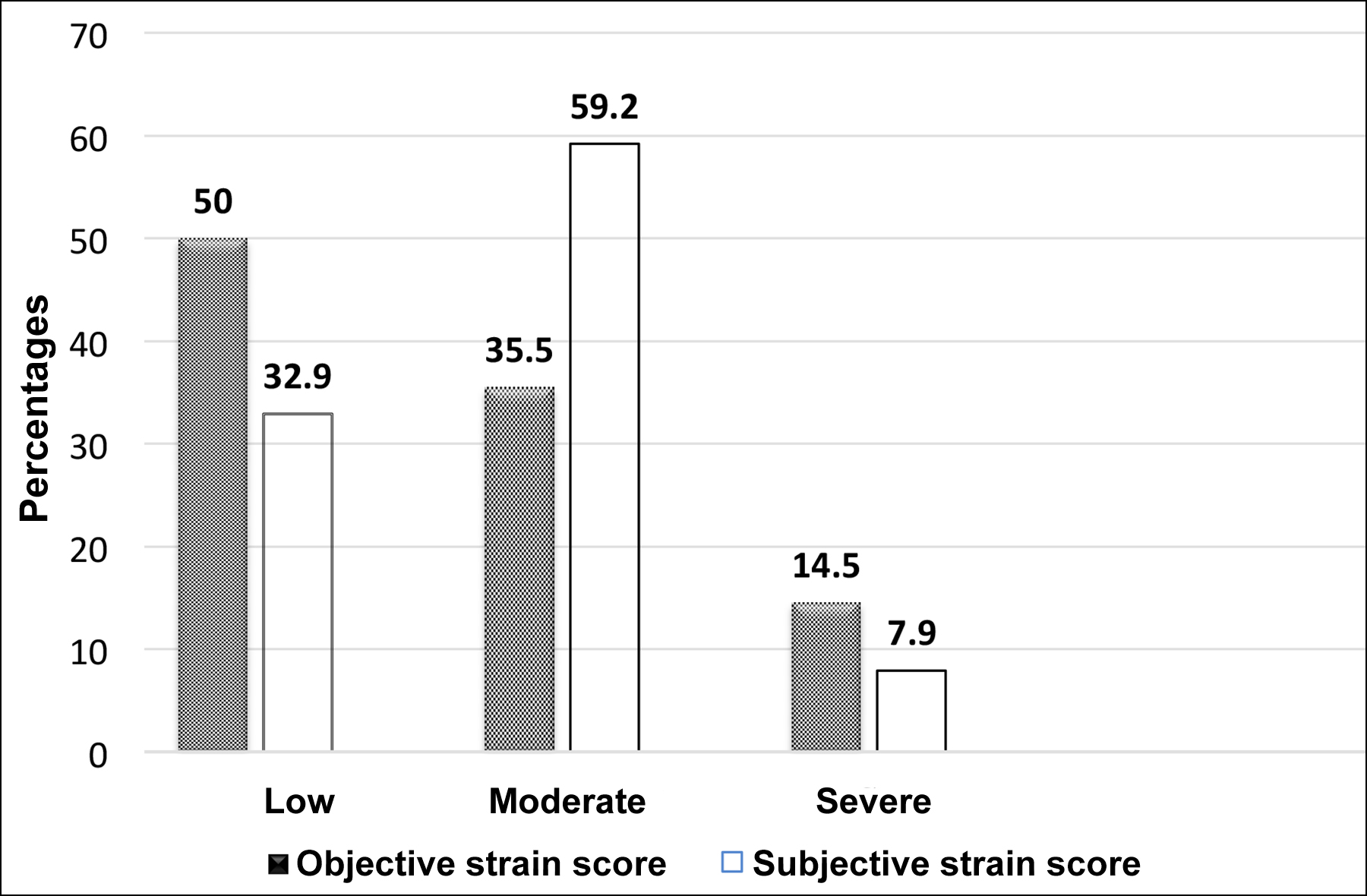 Figure 1: Objective and Subjective strain scores among the study participants.
Figure 1: Objective and Subjective strain scores among the study participants.
Table I: Association of demographic variables with subjective and objective strain scores.
|
Variables |
Subjective strain scores |
p-value |
Objective strain scores |
p-value |
||||
|
Low |
Moderate |
Severe |
Low |
Moderate |
Severe |
|||
|
Age |
|
0.461 |
|
0.862 |
||||
|
25-35 years |
12 (48.0%) |
22 (48.9%) |
3 (50%) |
18 (47.4%) |
13 (48.1%) |
6 (54.5%) |
||
|
36-45 years |
9 (36.0%) |
19 (42.2%) |
1 (16.7%) |
13 (34.2%) |
12 (44.4%) |
4 (36.4%) |
||
|
46-55 years |
3 (12.0%) |
4 (8.9%) |
2 (33.3%) |
6 (15.8%) |
2 (7.4%) |
1 (9.1%) |
||
|
56 and above |
1 (4%) |
0 (0%) |
0 (0%) |
1 (2.6%) |
0 (0%) |
0 (0%) |
||
|
Gender |
|
0.016 |
|
0.152 |
||||
|
Male |
9 (36.0%) |
4 (8.9%) |
2 (33.3%) |
10 (26.3%) |
5 (18.5%) |
0 (0%) |
||
|
Female |
16 (64.0%) |
41 (91.1%) |
4 (66.7%) |
28 (73.7%) |
22 (81.5%) |
11 (100.0%) |
||
|
Education |
|
0.459 |
|
0.279 |
||||
|
Not formally educated |
1 (4.0%) |
0 (0%) |
0 (0%) |
1 (2.6%) |
0 (0%) |
0 (0%) |
||
|
Secondary |
1 (4.0%) |
2 (4.4%) |
0 (0%) |
2 (5.3%) |
1 (3.7%) |
0 (0%) |
||
|
Intermediate |
1 (4.0%) |
6 (13.3%) |
0 (0%) |
6 (15.8%) |
0 (0%) |
1 (9.1%) |
||
|
Graduate |
10 (40.0%) |
20 (44.4%) |
5 (83.3%) |
16 (42.1%) |
16 (59.3%) |
3 (27.3%) |
||
|
Postgraduate |
12 (48.0%) |
17 (37.8%) |
1 (16.7%) |
13 (34.2%) |
10 (37.0%) |
7 (63.6%) |
||
|
Occupation |
|
0.299 |
|
|
|
0.269 |
||
|
Businessmen |
2 (8.0%) |
3 (6.7%) |
1 (16.7%) |
4 (10.5%) |
2 (7.4%) |
0 (0%) |
||
|
Professional |
9 (36.0%) |
6 (13.3%) |
1 (16.7%) |
9 (23.7%) |
7 (25.9%) |
0 (0%) |
||
|
Home maker |
12 (48.0%) |
34 (75.6%) |
4 (66.7%) |
22 (57.9%) |
18 (66.7%) |
10 (90.9%) |
||
|
Others |
2 (8.0%) |
2 (4.4%) |
0 (0%) |
3 (7.9%) |
0 (0%) |
1 (9.1%) |
||
|
Descriptive statistics for frequencies and chi-square test for p-values were applied. |
||||||||
Table II: Association of demographic variables with externalised and internalised subjective strain scores.
|
Variables |
Externalised subjective strain score |
p-value |
Internalised subjective strain score |
p-value |
||||
|
Low |
Moderate |
Severe |
Low |
Moderate |
Severe |
|||
|
Age |
|
0.937 |
|
0.324 |
||||
|
25-35 years |
28 (47.5%) |
9 (52.9%) |
- |
8 (50.0%) |
14 (42.4%) |
15 (55.6%) |
||
|
36-45 years |
23 (39.0%) |
6 (35.3%) |
- |
4 (25.0%) |
16 (48.5%) |
9 (33.3%) |
||
|
46-55 years |
7 (11.9%) |
2 (11.8%) |
- |
3 (18.8%) |
3 (9.1%) |
3 (11.1%) |
||
|
56 and above |
1 (1.7%) |
0 (0%) |
- |
1 (6.3%) |
0 (0%) |
0 (0%) |
||
|
Gender |
|
0.656 |
|
0.002 |
||||
|
Male |
11 (18.6%) |
4 (23.5%) |
- |
8 (50.0%) |
5 (15.2%) |
2 (7.4%) |
||
|
Female |
48 (81.4%) |
13 (76.5%) |
- |
8 (50.0%) |
28 (84.8%) |
25 (92.6%) |
||
|
Education |
|
0.296 |
|
0.625 |
||||
|
Not formally educated |
1 (1.7%) |
0 (0%) |
- |
0 (0%) |
1 (3.0%) |
0 (0.0%) |
||
|
Secondary |
3 (5.1%) |
0 (0%) |
- |
1 (6.3%) |
1 (3.0%) |
1 (3.7%) |
||
|
Intermediate |
7 (11.9%) |
0 (0%) |
- |
1 (6.3%) |
5 (15.2%) |
1 (3.7%) |
||
|
Graduate |
24 (40.7%) |
11 (64.7%) |
- |
6 (37.5%) |
13 (39.4%) |
16 (59.3%) |
||
|
Postgraduate |
24 (40.7%) |
6 (35.3%) |
- |
8 (50.0%) |
13 (39.4%) |
9 (33.3%) |
||
|
Occupation |
|
0.704 |
|
0.188 |
||||
|
Businessmen |
5 (8.5%) |
1 (5.9%) |
- |
|
2 (12.5%) |
3 (9.1%) |
1 (3.7%) |
|
|
Professional |
14 (23.7%) |
2 (11.8%) |
- |
6 (37.5%) |
8 (24.2%) |
2 (7.4%) |
||
|
Homemaker |
37 (62.7%) |
13 (76.5%) |
- |
7 (43.8%) |
20 (60.6%) |
23 (85.2%) |
||
|
Others |
3 (5.1%) |
1 (5.9%) |
- |
1 (6.3%) |
2 (6.1%) |
1 (3.7%) |
||
|
Sole Caregiver |
0.097 |
|
0.129 |
|||||
|
Yes |
26(44%) |
12(70.58%) |
- |
5(31.25%) |
16(48.48%) |
17(62.96%) |
|
|
|
No |
33(55.9%) |
5(29.41%) |
- |
11(68.75%) |
17(51051%) |
10(37.03%) |
||
The overall caregiver strain was reported to be severe by 11.8% (n=9), moderate by 47.4% (n=36), and low by 40.8% (n=31) of participants. There was no association of any of the demographic variables with the overall strain scores.
About 50% of the participants reported low in objective strain whereas 59.2% of the participants subjectively felt the strain to be moderate level (Figure 1). A significant association was found between the gender of the participants and the subjective strain (p=0.016); however, no significant association was found between demographics and objective strain (Table I). There is an association of the gender of participants with internalised subjective strain (p=0.002, Table II).
DISCUSSION
It is already well-established fact that the parents and caregivers of children with autism lead a stressful life. They are more prone to develop psychiatric problems thus affecting their relationship with the child, the caregiving role, and ultimately child-rearing. The results of this study add to preexisting literature presenting greater levels of stress among caregivers who take care of a child with ASD. The present finding is much close to the previous findings on caregivers of children with Autism in other parts of the world.18 An important finding in this study was a positive correlation between the gender of the participant and subjective strain where mothers reported perceived stress more than what was depicted objectively. This finding points towards the fulfilment of responsibility which females undertake as a part of gender-role in Pakistani culture despite feeling stressed and unwell. Even the caregiving mothers must conform to their role as a caretaker of the household in addition to the added responsibility of attending to a special needs child, mostly without support. Another finding in this study is a positive correlation between gender and internalised subjective strain. This finding, again, culturally co-relates to the feelings of worry, guilt, and fatigue which mothers experience despite single-handedly trying to juggle with multiple roles at the same time. This study further identifies a link between sole caregiver and externalised subjective strain which suggests that being the only caregiver may give rise to feelings of anger and embarrassment. Interestingly, no correlation was seen between the attendance of special schools or therapy centres with objective caregiver strain. Moreover, no correlation was found between the occupation of the caregiver and the caregiving strain. Similarly, neither the age of the patient or the age of the caregiver was found to have an association with the caregiver strain.
Since Pakistan is a country with limited resources and poor social determinants of mental health, healthcare is out of pocket, and there is a stigma to seeking help, alongside significant expectations from mothers to indulge in caregiving without self-care time. The results of this study highlight the need for family interventions that address strategies to empower the caregivers of patients with ASD which would eventually enhance the quality of life of both the parents as well as the patients. In a collectivistic society like Pakistan, empathy and support in the form of a joint family could help divide chores and provide respite to the primary caregiver while another member momentarily attends to the patient’s needs. The authors proposed that regular caregiver screening and provision of a helping hand in the house to divide the caregiving responsibilities is a possible way for managing and decreasing the level of strain.
Although other independent variables are insignificant to strain rated in these caregivers, there is a probability that such results are due to the limited sample size and the presence of confounders, which cannot be adjusted due to the study design limitation. In view of the increasing burden on the parents due to this lifelong illness, it is strongly recommended to devise approaches aimed at supporting caregivers, ultimately leading to improvement of the quality of life of both the patients as well as their caregivers. Social support for the parents of autistic children has been shown to greatly influence self-reported levels of stress by the mothers19 leading to a need for the implementation of organised social support programs for such parents and caregivers.20
The major limitation of this study is the limited sample size and use of a single study setting. The result cannot be generalised overall irrespective of the fact that the study centre provides services cross-culturally. There remains a possibility of relevant details to have fallen short in a single interview. The study design used has its own limitations, as it does not provide room to exclude confounders, for example, selection bias or any other stressors unrelated to the caregiving role may have contributed to the results, which may have affected the outcome significantly. It also does not establish grounds to indicate causation between the dependent variables.
CONCLUSION
Parenting an autistic child involves challenges and demands support. Caregiver strain can be a debilitating condition for the sufferer, especially if it is moderate to severe in intensity. This study indicates a high frequency of moderate strain affecting 47.4% of the caregivers irrespective of the gender or duration of caregiving. However, it also suggests that support from other family members can act as a protective factor in the caregiving process.
ETHICAL APPROVAL:
Ethical approval was obtained from The Aga Khan University Hospital's Ethical Review Committee (reference number 2019-1673- 4089).
PATIENTS’ CONSENT:
All participants provided written consent.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
RA, TN: Conceived the study and were involved in process mapping.
RA: Involved in the data collection, interpretation, and drafting.
SP: Gave substantial contribution to interpretation of data and write-up of the manuscript.
RA, MM: Reviewed and revised the manuscript for important intellectual content.
RA, TN, MM: Critically reviewed and edited the final manu-script.
All the authors have approved the final version of the manu-script to be published.
REFERENCES
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, Fifth Edition. Washington, DC; 2013.
- Zeidan J, Fombonne E, Scorah J, Ibrahim A, Durkin MS, Saxena S, et al. Global prevalence of autism: A systematic review update. Autism Research 2022; 15(5):778-90. doi.org/10.1002/aur.2696.
- Hossain MD, Ahmed HU, Jalal Uddin MM, Chowdhury WA, Iqbal MS, Kabir RI, et al. Autism spectrum disorders (ASD) in South Asia: A systematic review. BMC Psychiatry 2017; 17(1):1-7. doi: 10.1186/s12888-017-1440-x.
- Poovathinal SA, Anitha A, Thomas R, Kaniamattam M, Melempatt N, Anilkumar A, et al. Prevalence of autism spectrum disorders in a semiurban community in south India. Ann Epidemiol 2016; 26(9):663-5. doi: 10.1016/j.annepidem.2016.07.003.
- Khalid M, Raza HM, Driessen TJ, Lee P, Tejwani L, Sami A, et al. Genetic risk of autism spectrum disorder in a Pakistani population. Genes 2020, 11(10):1206. doi.org/10.1016/j.annepidem.2016.07.003.
- Drahota A, Aarons GA, Stahmer AC. Developing the autism model of implementation for autism spectrum disorder community providers: study protocol. Implement Sci 2012; 7(1):85. doi.org/10.1186/1748-5908-7-85.
- Kanne SM, Mazurek MO. Aggression in children and adolescents with ASD: Prevalence and risk factors. J Autism Dev Disord 2011; 41(7):926-37. doi: 10.1007/s10803-010-1118-4.
- Szatmari P, Chawarska K, Dawson G, Georgiades S, Landa R, Lord C, et al. Prospective longitudinal studies of infant siblings of children with autism: Lessons learned and future directions. J Am Academy Child Adolescent Psychiatry 2016; 55(3):179-87. doi: 10.1016/j.jaac.2015.12.014.
- Zwaigenbaum L, Bryson SE, Brian J, Smith IM, Roberts W, Szatmari P, et al. Stability of diagnostic assessment for autism spectrum disorder between 18 and 36 months in a high‐risk cohort. Autism Res 2016; 9(7):790-800. doi: 10. 1002/aur.1585.
- Werling DM, Parikshak NN, Geschwind DH. Gene expression in human brain implicates sexually dimorphic pathways in autism spectrum disorders. Nature Commun 2016; 7:10717. doi: 10.1038/ncomms10717.
- Parks SM, Novielli KD. A practical guide to caring for caregivers. Am Fam Physician 2000; 62(12):2613-22. PMID: 11142468.
- Gitlin LN, Belle SH, Burgio LD, Czaja SJ, Mahoney D, Gallagher-Thompson D, et al. Effect of multicomponent interventions on caregiver burden and depression: The reach multisite initiative at 6-month follow-up. Psychol Aging 2003; 18(3):361. doi: 10.1037/0882-7974.18.3.361.
- Parrish MM, Adams S. Caregiver comorbidity and the ability to manage stress. J Gerontol Soc Work 2004; 42(1):41-58. doi.org/10.1300/J083v42n01_04.
- Leff PT, Walizer EH. The uncommon wisdom of parents at the moment of diagnosis. Family Systems Med 1992; 10(2):147. doi.org/10.1037/h0089203.
- Shanthi C, rao Sireesha S, Kuna SR. A cross sectional study of caregiver burden and psychiatric morbidity in primary caregivers of mentally retarded subjects. Sch J App Med Sci 2015; 3(3C):1199-205.
- Brannan A, Heflinger C, Bickman L. The caregiver strain questionnaire: Easuring the impact on the family of living with a child with serious emotional disturbance. J Emot Behav 1997; 5:212-22. doi.org/10.1177/106342669700 500404.
- Khanna R, Madhavan SS, Smith MJ, Tworek C, Patrick JH, Becker-Cottrill B. Psychometric properties of the caregiver strain questionnaire (CGSQ) among caregivers of children with autism. Autism 2012; 16(2):179-99. doi:10.1136/ gpsych-2020-100246.
- Bromley J, Hare DJ, Davison K, Emerson E. Mothers supporting children with autistic spectrum disorders social support, mental health status and satisfaction with services. Autism 2004; 8(4):409-23. doi: 10.1177/1362 36130404 7224.
- Bitsika V, Sharpley CF. Stress, anxiety and depression among parents of children with autism spectrum disorder. Aust J Guidance Counsel 2004; 14(2):151-61. doi: 10.2147/ NDT.S107103.
- Daniels JL, Forssen U, Hultman CM, Cnattingius S, Savitz DA, Feychting M, et al. Parental psychiatric disorders associated with autism spectrum disorders in the offspring. Pediatrics 2008; 121(5):e1357-62. doi: 10.1542/ peds.2007-2296.