A Rare Cause of Recurrent Melena: Haemangioma of the Small Intestine
By Feng Chi, Yuefu Lan, Liangxian JiangAffiliations
doi: 10.29271/jcpsp.2022.08.1100Sir,
Haemangiomas of the small intestine are rare benign vascular neoplasms, representing 7%-10% of all benign small intestinal tumours.1 According to the size of the constituent vessels, they are histologically classified as cavernous, capillary, or mixed types; cavernous type is the most common.2
Gastrointestinal bleeding, either overt or occult, is the most common presentation of small intestinal haemangiomas. Less common presentations include intestinal obstruction, intussusception, and perforation.3 Capsule endoscopy is the first-line diagnostic modality, as it is pain-free and non-invasive.4 Other diagnostic modalities include the radiological examination and balloon-assisted enteroscopy. The ideal treatment is surgical resection.
A 62-year woman was admitted with complaints of recurrent melena for 6 months. The patient had no significant medical history, was not taking any medications, and did not have an unbalanced food intake. Physical examination was unremarkable except for pallor. Her haemoglobin was 7.5 g/dL and haematocrit, 25%. Gastroscopy revealed superficial gastritis and colonoscopy showed a normal result. Therefore, small intestinal bleeding was considered. Capsule endoscopy was carried out, but no bleeding was detected. Abdominal contrast-enhanced computed tomography was unrevealing. She was treated with oral iron supplementation but there was no diminution in the recurrence of melena.
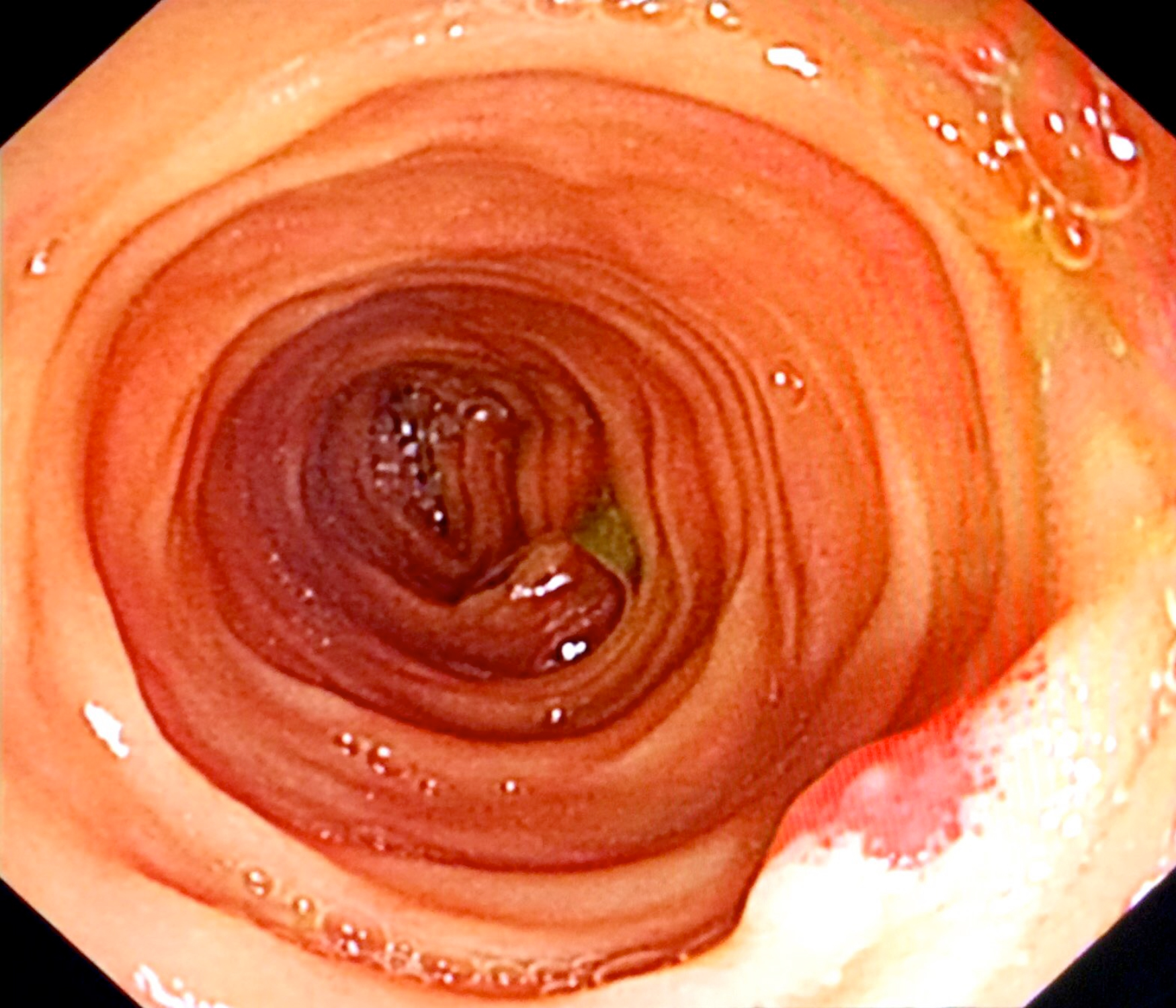 Figure 1: Intraoperative enteroscopy showing a polypoid lesion in the small intestine.
Figure 1: Intraoperative enteroscopy showing a polypoid lesion in the small intestine.
Finally, the patient underwent diagnostic laparoscopy and intraoperative enteroscopy. Initially, diagnostic laparoscopy was performed, which found that the small intestine was macroscopically normal. Then, the small intestine was extracted through a small abdominal incision. A sterilised enteroscope was inserted through an incision made at the juncture of the jejunum and ileum. The whole small intestine was examined, and a red protruding lesion of 0.5 cm in diameter was found in the ileum about 10 cm distal to the intestinal incision (Figure 1). The lesion was resected locally. The patient recovered uneventfully and was discharged on the sixth postoperative day. Histopathology identified the mass as a mixed capillary-cavernous haemangioma (Figure 2). During a 6 month follow-up, she remained asymptomatic and the last haemoglobin was 12.1 g/dL.
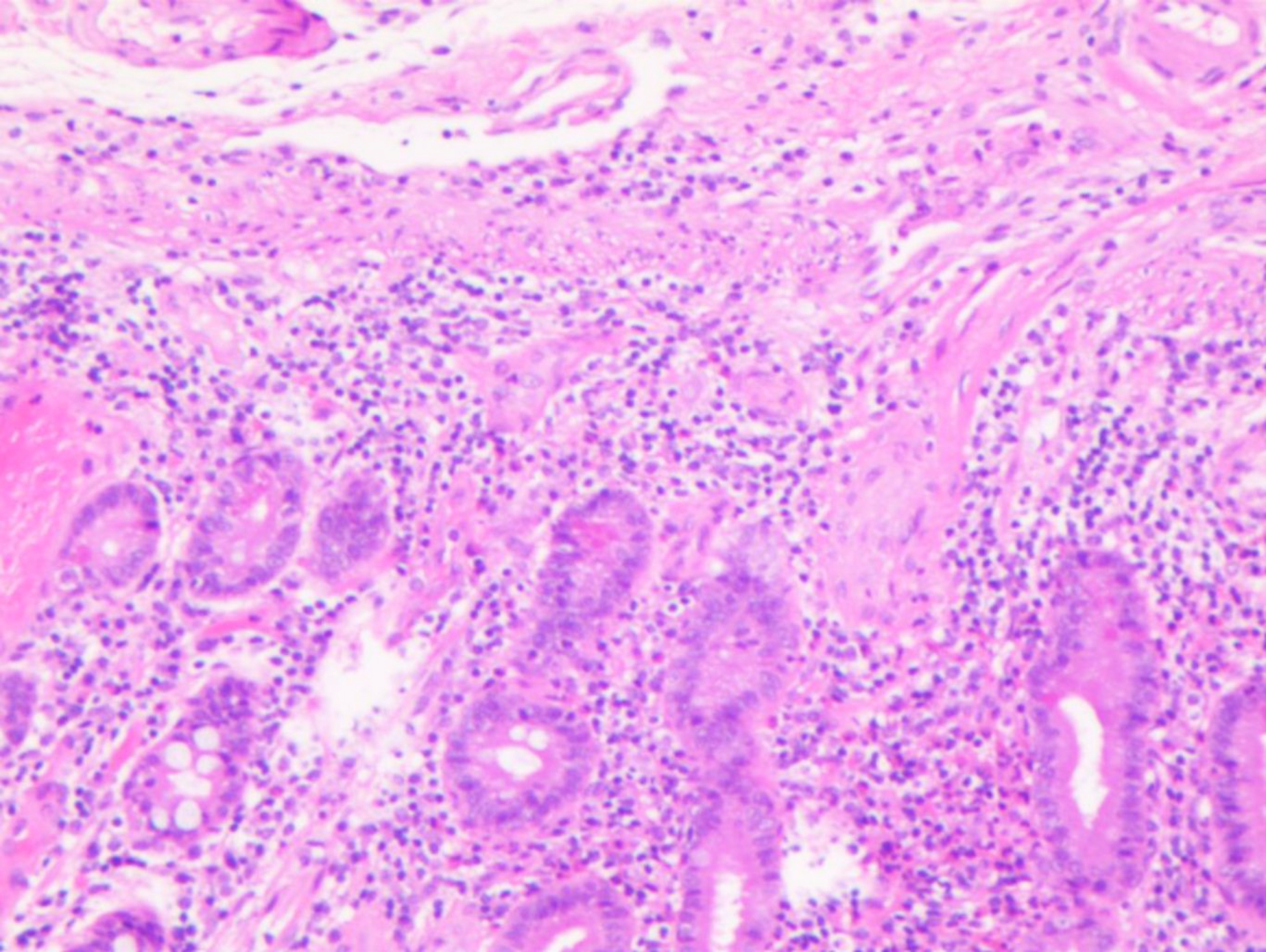 Figure 2: Micrograph of the lesion demonstrating proliferating capillaries and dilated cavernous vascular spaces (haematoxylin and eosin, ×100).
Figure 2: Micrograph of the lesion demonstrating proliferating capillaries and dilated cavernous vascular spaces (haematoxylin and eosin, ×100).
In recent years, capsule endoscopy and balloon-assisted enteroscopy have revolutionised small intestinal imaging studies and have improved the detection of obscure gastrointestinal bleeding sources. It was reported that 91.9% of small intestinal haemangiomas could be diagnosed by capsule endoscopy and/or balloon-assisted enteroscopy preoperatively.5 We present a case of small intestinal haemangioma in which intraoperative enteroscopy played an important role in identifying the location of the lesion which was missed by capsule endoscopy. Intraoperative enteroscopy should be recommended as a possible option in the accurate evaluation of the patients with small intestinal disorders, especially in cases where small intestinal bleeding sources are missed by capsule endoscopy and balloon-assisted enteroscopy.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
FC, YL: Surgery, paper writing and literature review.
LJ: Literature review and manuscript revision.
All authors approved the final version of the manuscript to be published.
REFERENCES
- Akazawa Y, Hiramatsu K, Nosaka T, Saito Y, Ozaki Y, Takahashi K, et al. Preoperative diagnosis of cavernous hemangioma presenting with melena using wireless capsule endoscopy of the small intestine. Endosc Int Open 2016; 4(3):E249-51. doi: 10.1055/s-0041-111321.
- Boyle L, Lack EE. Solitary cavernous hemangioma of small intestine. Case report and literature review. Arch Pathol Lab Med 1993; 117(9): 939-41.
- Durer C, Durer S, Sharbatji M, Comba IY, Aharoni I, Majeed U. Cavernous hemangioma of the small bowel: A case report and literature review. Cureus 2018; 10(8): e3113. doi: 10.7759/cureus.3113.
- Li XL, Shen JT, Li YP, Tang CW, Huang LB, Li CC, et al. Capsule endoscopy in diagnosis of small bowel diseases: A health technology assessment. J Evid Based Med 2014; 7(2): 84-102. doi: 10.1111/jebm.12095.
- Hu PF, Chen H, Wang XH, Wang WJ, Su N, Shi B. Small intestinal hemangioma: Endoscopic or surgical intervention? A case report and review of literature. World J Gastrointest Oncol 2018; 10(12):516-21. doi:10.4251/ wjgo.v10.i12.516.